|
SAMHSA Primer on Medicaid’s Role in BH Care
A recent resource from the Substance Abuse and Mental Health Services Administration (SAMHSA), “Medicaid Primer: An Overview of Medicaid and Behavioral Health,” is designed to help new staff within state behavioral health agencies understand Medicaid and its intersection with behavioral health to support stronger collaboration with state Medicaid agencies.
Medicaid is one of the largest payers of behavioral health care in the U.S., covering a significant share of individuals with mental health and substance use disorders—particularly those with low incomes or disabilities. It outlines how Medicaid helps fund a broad continuum of services, from outpatient care and medications to inpatient treatment and recovery supports, making it a foundational component of state behavioral health systems.
Based on input from current state behavioral health and Medicaid leaders, this document highlights effective strategies for partnering with Medicaid authorities to improve behavioral health care, including fostering cross-agency collaboration, and strengthening understanding of how Medicaid can expand access to services. Overall, the resource underscores the importance of Medicaid as both a financing mechanism and a policy lever, with future opportunities centered on improving coordination, expanding access, and strengthening the behavioral health workforce. |
|
CCBHCs Serving Veterans & Military Families
The Substance Abuse & Mental Health Services Administration (SAMHSA) has released a new Engaging Service Members, Veterans, and Families toolkit to help Certified Community Behavioral Health Clinics (CCBHCs) strengthen engagement and improve support for military-connected communities.
The resource highlights the unique challenges faced by service members, veterans, and their families—including stigma, cultural differences, and system navigation barriers—and emphasizes the importance of culturally competent, coordinated care. It positions CCBHCs as key access points for delivering integrated, community-based behavioral health services tailored to these populations.
The toolkit outlines practical strategies to strengthen engagement, including building military cultural competence among providers, developing partnerships with military and veteran-serving organizations, and integrating peer support and family-centered approaches into care delivery. It also emphasizes the importance of outreach, screening, and care coordination to ensure individuals are connected to appropriate services across systems. Overall, the resource underscores the need for more intentional, culturally responsive approaches to improve access, trust, and outcomes for service members, veterans, and their families within the behavioral health system.
View the full toolkit here. |
|
SAMHSA Advisory on CHW and Peer Supporters in Bridging BH Deserts
A new advisory from the Substance Abuse and Mental Health Services Administration (SAMHSA), “Expanding Behavioral Health Teams in Care Deserts With Community Health Workers and Peer Support Specialists,” examines strategies to address widespread gaps in access to behavioral health services. The report notes that millions of Americans live in “care deserts,” where shortages of providers, long wait times, and high costs limit access to treatment for mental health and substance use disorders. To address these gaps, the advisory highlights the potential of integrating community health workers and peer support specialists—trusted, community-based providers—to extend the reach of behavioral health services and improve engagement in care.
The advisory identifies several key strategies for expanding access in underserved communities, including:
- Leveraging community health workers and peer support specialists to provide culturally responsive, community-based care and outreach.
- Using these roles to bridge gaps between clinical providers and communities, improving trust, engagement, and care navigation.
- Expanding workforce capacity by incorporating non-clinical providers to address shortages in licensed behavioral health professionals.
- Integrating peer and community-based supports across the continuum of care, from prevention and early intervention to treatment and recovery.
The findings highlight a growing emphasis on workforce innovation as a strategy to improve access to behavioral health care, particularly in rural and underserved areas. The advisory suggests that expanding the use of community-based providers may help reduce disparities, improve outcomes, and strengthen system capacity without relying solely on traditional clinical workforce expansion. Looking ahead, the report points to the importance of policy alignment, sustainable funding, and training infrastructure to support these roles, positioning them as a key component of efforts to close behavioral health care gaps and build more accessible, community-centered systems of care. |
|
SAMHSA Recovery Housing Funding
SAMHSA's Center for Financing Reform and Innovation (CFRI) released their new report on “Recovery Housing: Funding Sources and Financial Sustainability – Insights from NARR-Certified Recovery Residences”. The report and webinar summarize the investigation on how states can effectively expand access to recovery housing and identifies trends in recovery housing financing, sustainable funding sources and opportunities for expansion.
Recovery housing, which is structured, peer-supported living environments for individuals in recovery, has been associated with improved outcomes, including reduced substance use, lower rates of relapse and incarceration, and increased employment and income. Despite these benefits, the report emphasizes that securing stable and sustainable funding remains one of the primary barriers to expanding access and maintaining these services over time.
The report outlines a range of funding sources currently used to support recovery housing, including federal and state grants, Medicaid and other public funding streams, resident fees, and private or philanthropic contributions. However, no single funding source is sufficient on its own, requiring providers to braid multiple funding streams together to maintain operations and scale services. SAMHSA highlights the importance of aligning policies, improving cross-sector collaboration, and developing clearer financing strategies to support both housing infrastructure and service delivery. |
|
Psilocybin Use Increases in States Following Decriminalization
A recent study published in JAMA, “Psilocybin Trends in States that Decriminalized Use”, examines how psilocybin use changed in Oregon and Colorado after decriminalization. The study found that past-year psilocybin use increased in both states following policy changes, outpacing national trends. While psilocybin use has been rising across the U.S. more broadly, the findings suggest that state-level decriminalization may be associated with additional increases beyond these existing trends.
The study highlights several key findings related to use-patterns, including:
- Increases in 12-month psilocybin use in both Oregon and Colorado after decriminalization.
- Growth in use that exceeded national increases during the same time period.
- Broader national trends showing rising psychedelic use, suggesting multiple contributing factors beyond policy changes alone.
- Limited evidence to fully isolate the causal impact of decriminalization from other cultural and clinical influences.
The findings highlight the evolving landscape of psychedelic use as states adopt new policy approaches. The study suggests a need for continued monitoring of use patterns, public health impacts, and potential risks as access expands. Looking ahead, policymakers and health systems may need to balance emerging therapeutic interest in psilocybin with appropriate safeguards, education, and data collection to better understand its population-level effects. |
|
Higher & Earlier Methadone Doses Linked to Better Treatment Stays
A recent study published in JAMA Network Open, “Methadone Dose and Patient-Directed Discharge in Hospitalized Patients With Opioid Use Disorder,” found that higher cumulative doses of methadone administered within the first 24 to 48 hours of hospitalization were associated with a significantly lower likelihood of patient-directed discharge. Given that 10% to 20% of hospitalizations for patients with opioid use disorder (OUD) end prematurely, and are linked to worse health outcomes, these findings highlight the role of early withdrawal management in improving patient retention and care continuity.
The study identifies several key factors influencing these outcomes, including:
- Higher methadone doses in the first 24 hours were consistently associated with reduced odds of patient-directed discharge across multiple time points.
- Untreated withdrawal symptoms and pain are commonly cited reasons for early discharge, underscoring the importance of timely and adequate symptom management.
- Despite evidence supporting medications for opioid use disorder (MOUD), only a minority of hospitalized patients receive these treatments, reflecting persistent gaps in clinical practice.
- Existing hospital policies and clinical norms—many developed prior to the rise of fentanyl—may limit appropriate dosing and delay effective treatment initiation.
The findings suggest an opportunity to re-evaluate current hospital protocols for treating opioid withdrawal, particularly in the context of the fentanyl-driven overdose crisis. Expanding access to early, adequately dosed methadone treatment may improve patient retention, reduce adverse outcomes associated with incomplete care, and strengthen the role of hospitalization as a key intervention point for initiating addiction treatment. For policymakers and health systems, this study reinforces the importance of aligning clinical guidelines, provider training, and hospital policies with emerging evidence to better meet the needs of patients with OUD. |
|
SNAP Benefit Cuts Could Lead to Tens of Thousands of Avoidable Deaths
A recent analysis from the Center for American Progress has found that the expanded work requirements and other policy changes related to the Supplemental Nutrition Assistance Program (SNAP) could result in millions of individuals losing access to food assistance, with an estimated 70,000 avoidable deaths over time. The analysis emphasizes the well-established connection between food insecurity and adverse health outcomes, including higher rates of chronic disease, worsened mental health, and increased mortality risk.
The report identifies several key drivers contributing to these projected outcomes, including:
- Expanded work requirements that could lead to significant coverage losses among low-income adults.
- Loss of consistent access to nutritious food, which is strongly associated with poorer health outcomes and increased risk of premature death.
- Disproportionate impacts on vulnerable populations, including individuals with low incomes, unstable employment, or existing health conditions.
- State-level variation in impacts, with some regions expected to experience higher rates of benefit loss and associated health consequences.
The findings underscore the significant role that nutrition assistance programs play in supporting population health and preventing avoidable mortality. The report suggests that reductions in SNAP benefits may increase strain on healthcare systems, worsen health disparities, and shift costs to other public systems. Looking ahead, the analysis highlights the importance of considering the health implications of nutrition policy decisions and aligning program design with evidence linking food access to long-term health and economic stability. |
|
OIG Finds CVS Overbilled $600M for Rx Benefits of Federal Employees
A new audit report issued by the U.S. Office of Personnel Management (OPM), Office of the Inspector General (OIG) has accused a drug middleman owned by CVS Health of overbilling a program that covers 9 million federal employees by $615 million over a four-year period. The findings occurred across all years of the audit scope, which ranged between 2018-2021.
Specifically, the audit found the following three findings for corrective action:
- The PBM did not pass through the discounts it negotiated with two of the largest retail pharmacy chains, resulting in nearly a $479M overcharge to the Carrier and the Federal Employees Health Benefits Program (FEHBP).
- The PBM failed to return nearly $109M in credits for transmission fees that it collected from retail pharmacies to process the Carrier’s prescription drug benefits. Instead of passing through these credits, the PBM charged the FEHBP a higher amount than was actually paid to the retail pharmacies.
- The Carrier overcharged the FEHBP almost $27M by paying the PBM an incentive based on a percentage of their excess savings above the retail claims pricing guarantee between the Carrier and the PBM in 2018, 2019, and 2021.
The OIG has recommended that the OPM demand that CVS repay about $600M. The move furthers longstanding scrutiny about the oversaturation of PBMs that critics say control the market to decide which drugs insurance will cover, and ultimately drive-up prices for life-saving drugs. Currently, the largest three PBMs control nearly 80% of the insured drug transactions. |
|
OIG Investigation Cites Overuse of Antipsychotic Drugs in Nursing Homes
A new report issued by the U.S. Department of Health & Human Services (HHS) Office of the Inspector General (OIG), “Nursing Homes’ Inappropriate Use of Antipsychotic Drugs Poses a Risk to Residents”, found that these while medications are intended for specific psychiatric conditions, they are frequently administered to residents with dementia, despite not being approved for this use and carrying FDA warnings of increased mortality risk. In many cases, antipsychotics were used to manage behavioral symptoms such as agitation or confusion, raising concerns about their role as behavioral management tools rather than clinically necessary treatments.
The report identifies several systemic gaps contributing to inappropriate use, including:
- Nursing homes often ignoring required safeguards, such as attempting non-pharmacological interventions, monitoring side effects, or reducing dosages over time.
- Key oversight roles like medical directors and consulting pharmacists, were not consistently effective in identifying or preventing inappropriate prescribing.
- Facility-level policies and procedures are often insufficient to ensure compliance with federal standards.
These findings mirror recent trends identified in a cross-sectional study recently released by JAMA, that found that between 2013 and 2023, the proportion of antipsychotic prescriptions written by registered nurses and physician assistants in nursing homes increased from 13.8% to 39.6%, making them the largest group of prescribers. While during that same period, the proportion of antipsychotic prescriptions written by psychiatrists decreased from 48.4% to 32.4%, and by primary care physicians reduced from 33.0% to 23.8%.
The OIG report underscores the need for strengthened oversight, clearer accountability, and more consistent implementation of evidence-based care practices. OIG recommends that CMS expand transparency efforts, reinforce the responsibilities of medical directors and pharmacists, and support facilities in improving internal policies related to antipsychotic use. Looking ahead, these findings suggest a likely shift toward more rigorous monitoring, greater emphasis on non-pharmacological dementia care, and potential policy or regulatory adjustments to better align incentives with quality care outcomes. For healthcare systems and policymakers, the report highlights the importance of balancing clinical discretion with stronger safeguards to ensure that medication use prioritizes resident safety and well-being. |
|
Vorys Releases White Paper on Preparing for State Medicaid Audits
Following a recent webinar, Vorys, Sater, Seymour and Pease LLP has released a white paper summarizing key insights to help you prepare for Ohio Auditor of State Medicaid Compliance Examinations, focusing on what providers can expect, how to prepare, and the trends emerging from the Auditor’s recent reviews.
The Ohio Auditor of State (the Auditor) conducts Medicaid compliance examinations (commonly referred to as audits), to identify improper payments and to ensure compliance with Medicaid reimbursement requirements. These audits are unique from other provider post-payment reviews — they follow a particular process. Their findings are ultimately public and, therefore, can have significant financial and reputational effects on the provider. Vorys recommends that provider organization not navigate that alone. With the current emphasis on waste, fraud, and abuse mitigation efforts increasing, providers are recommended to take proactive steps to prepare now.
Key insights include:
- How the Auditor conducts Medicaid compliance examinations and the strict timelines providers must meet
- Common documentation and billing issues identified during 2025 behavioral health audits
- The Auditor’s increasing use of data analytics and extrapolation to identify and expand findings
- Strategic steps providers should take — such as engaging experienced counsel early, preparing organized record submissions, and treating the final response like a legal brief—to reduce exposure and avoid adverse outcomes
Download the full white paper here. The webinar recording is available to view here. |
|
Opioid Deaths Dropped in 2024, Ohio’s Decline was Even Steeper
According to a new KFF report, opioid overdose deaths in the U.S. fell sharply from 2023 to 2024. Nationally, the total number of deaths dropped nearly 32%, from about 79,000 in 2023 to 54,000 in 2024.
Ohio’s drop was even steeper, with deaths falling about 45% from nearly 4,000 in 2023 to about 2,200 in 2024. The state’s opioid overdose death rate was 20.1 per 100,000 population in 2024.
West Virginia in 2024 had the highest opioid death rate (38.6 per 100,000) among U.S. states. Nebraska had the lowest rate at 3.3 per 100,000 population.
Fentanyl was involved in most opioid deaths in 2024. Despite this, declines in fentanyl-involved deaths drove the overall drop in opioid deaths. Deaths involved other opioids, including opioids and heroin, also declined but to a lesser extent. |
|
RFA Due Apr 20th: Assisted Outpatient Tx Funding
The Substance Abuse and Mental Health Services Administration (SAMHSA) has issued a Notice of Funding Opportunity (SM-26-001) for the development and implementation of Assisted Outpatient Treatment (AOT) programs.
This opportunity is available to organizations that have not previously implemented an AOT program and is intended to support jurisdictions in establishing community-based AOT services that work collaboratively with civil courts, behavioral health providers, and other local partners. Programs funded through this opportunity are expected to align with state AOT laws and guidance while supporting individuals with serious mental illness in the community.
SAMHSA anticipates awards of up to $500,000 per year for programs serving 50 patients or fewer and up to $750,000 per year for programs serving more than 50 patients. The deadline to apply is April 20. Read the full NOFO here.
DBH is available to support interested applicants and community partners by providing technical assistance related to AOT program planning and implementation letters of support for organizations preparing to apply. Please contact [email protected] to request technical assistance or a letter of support. |
|
RFA Due Apr 20th: Implementing Zero Suicide in Health Systems
The Substance Abuse and Mental Health Services Administration (SAMHSA) has issued a Notice of Funding Opportunity for the “Implementing Zero Suicide in Health Systems” grant.
The purpose of this program is to provide resources to healthcare systems for implementing the Zero Suicide framework for adults who are at risk of suicide. SAMHSA anticipates awarding at least 31 awards for an anticipated $400k - $700k for a project period of up to 5 years.
The deadline to apply is Monday, April 20th, 2026. For additional information, view the NOFO here. For questions related to this opportunity, contact Whitcomb Wakefield-Terpening at 240-276-2911 or by email at [email protected]. |
|
RFA Due Apr 20th: Children’s Mental Health Initiative
The Substance Abuse and Mental Health Services Administration (SAMHSA) has issued a Notice of Funding Opportunity for the “Children’s Mental Health Initiative” grant.
The purpose of the Children’s Mental Health Initiative program is to provide comprehensive community mental health services to children, youth, and young adults, birth through age 21 with a serious emotional disturbance, which may include efforts to identify and serve children at risk, and their families. SAMHSA anticipates awarding at least 22 awards for an anticipated $1M - $3M for a project period of up to 4 years.
The deadline to apply is Monday, April 20th, 2026. For additional information, view the NOFO here. For questions related to this opportunity, contact Kate Perrotta at 240-276-1903 or by email at [email protected]. |
|
RFA Due Apr 14th: Responsible Fatherhood Initiatives
The Ohio Commission on Fatherhood (OCF), through the Ohio Department of Children and Families (DCY), is seeking applicants for its SFY 2027 Responsible Fatherhood Initiative: Strong Fathers, Strong Families grants. The initiative will provide fathers with resources, support, and encouragement to enhance their parenting role.
DCY will award a total of $8.1 million annually to support services across 54 counties. Funding is set at $150,000 per county for the state fiscal year. Each application must clearly identify the specific county to be served with a maximum of up to two counties per applicant. The deadline to submit an application is April 14.
Questions? Email [email protected]
Learn more and apply here. |
|
Ohio General Assembly
This week state lawmakers completed their pre-primary legislative session and will not return until mid-May. Upon returning they will focus on approving a Capital Budget and finishing any key legislative priorities prior to the general election. We anticipate a continued focus on the Medicaid program and additional scrutiny on “fraud, waste and abuse” in healthcare programs. Because this year is an election year, lawmakers will be away from the statehouse most of the summer and fall until after the November general election. Of course, Ohio Council staff will continue to review and monitor legislative activity, engage lawmakers, and key staff, and advocate with DeWine administration officials on policy issues that affect the community behavioral health system. Accordingly, below are legislative measures that we have identified for further review and monitoring.
|
Bill
|
Bill Sponsor and Description
|
Current Status
|
|
HB 28
|
ELIMINATE REPLACEMENT PROPERTY TAX LEVY AUTHORITY (MATHEWS A, HALL T) To eliminate the authority to levy replacement property tax levies.
- Concerned about impact on local levies
- Included in Budget Bill
- House and Senate voted to override Gov’s veto
|
4/8/25 – Passed House, Pending in Senate Committee
*Included in HB 96
10/2/25 veto overridden and now law.
|
|
HB 58
(Changed from opposition to IP)
|
RECOVERY HOUSING Reform (PIZZULLI J, JARRELLS D) To reform regulatory system of recovery housing residences.
- Amended bill passed the House with positive amendment: removes certificate of need; bed fees; and ADAMHS board investigations of recovery residences. Enhances local law enforcement and requires more transparency and communication between ORH and DBH.
|
2/25/26 – Passed House w/ unanimous vote. 3/25/26 – Senate Community Revitalization (1st hearing)
|
|
HB 96
|
Operating Budget for SFY 26-27 (Stewart) to make appropriations for the biennium, levy taxes, and provide authorization for state programs.
- Passed GA 6/25; Gov Signed 6/30 – appropriations effective immediately; other provisions 9/30.
- Awaiting guidance on federal Medicaid changes (work requirements and redetermination process; MHAS block grants.
- Items not included Peers to CDPB; QMH credential; Tax increase on Marijuana and Sports Gaming
|
6/25/25–Enacted by General Assembly; 6/30/25-- Signed by Governor with 67 vetoes. Eff 9/30/25
10/2/25—GA voted to override one veto item (repeal of replacement levy)
|
|
HB 160
Consolidated into SB 56 conference committee report
11/19/25
|
REVISE LIQUOR CONTROL, HEMP, MARIJUANA LAWS (STEWART B) To revise specified provisions of the liquor control, hemp, and adult-use marijuana laws and to levy taxes on marijuana.
- Combines regulations and oversight responsibilities of recreational and medical marijuana into the Division of Marijuana Control (DMC).
- Reduces THC levels; imposes marketing, advertising and informational safeguards; prohibits use in public.
- Modifies how revenue from the 10% tax on adult-use marijuana is credited by dedicating 20% of the revenue to make temporary payments to municipalities and townships and redirecting the rest to the GRF.
Lawmakers to address in fall legislative session |
5/7/2025 - House Judiciary, (Third Hearing)
|
|
HB 162
|
Regarding Minors’ Medical Records (Click) Related to medical records of minors and parental consent.
- Requires a health care provider to ensure a minor’s parent or guardian has access to the minor’s EHR to the fullest extent permitted under HIPAA; and offer opportunities and reminders about consent.
|
10/15/2025 - PASSED HOUSE; 3/11/26 -Senate Health committee(1st hearing)
|
|
HB 172
(Oppose)
|
REQUIRE PARENTAL CONSENT-MINORS' MENTAL HEALTH SERVICE (NEWMAN J) To prohibit the provision of mental health services to minors without parental consent.
- Would repeal section 5122.04 (temporary emergency counseling authority)
- Teresa testified in opposition along with a host of other advocates
- Appears stalled in committee currently but monitoring for any activity or amendments.
|
11/19/2025 - House Health (Third hearing)
|
|
HB 184
|
Budget Corrections bill (NF reimbursement payment recalculation) (Stewart B) – originally a bill to address collegiate NIL contracts, the bill was used as the vehicle for a budget corrections bill.
See LSC summary
|
11/19/25 – Passed House and Senate. Sent to Governor for signature.
|
|
HB 189
|
REGARDING SCHOOL BEHAVIORAL THREAT MANAGEMENT (HALL T, GHANBARI H) Regarding a statewide behavioral threat management operational process for public and chartered nonpublic schools.
- Monitoring for significant changes and added requirements for providers working in schools
|
2/4/2026 - House Education (2nd hearing)
|
|
HB 190
|
PUBLIC SCHOOLS-GENDER PRONOUN USE (NEWMAN J, WILLIAMS J) To enact the Given Name Act regarding the use of gender pronouns in public schools.
- Monitoring for new requirements and possible penalties for providers operating in schools and working with students.
|
4/29/2025 - House Education (1st hearing)
|
|
HB 219
|
ESTABLISH INSURER NETWORK ADEQUACY STANDARDS (DEETER K) To establish network adequacy standards for health insurers.
*LSC Analysis
|
10/7/2025 - House Insurance, (Second Hearing)
|
|
HB 220
|
REGARDING PRIOR AUTHORIZATION REQUIREMENTS (WORKMAN H) Regarding health insurance and Medicaid program prior authorization requirements.
*Updated LSC analysis
SUMMARY
▪ Requires health insurance companies and ODM to
honor a prior authorization approval if a provider prescribes a change in dosage of the approved drug.
▪ Requires that the specialty and relevant qualifications of the clinical peer to be identified.
▪ Prohibits health insurers and ODM from charging a fee for appealing an adverse PA determination.
▪ Prohibits health insurers and ODM from retroactively denying a prior authorization for
mental health or substance use disorder treatment.
▪ Delays the bill’s effective date until January 1, 2028.
|
3/25/26 – Passed House (84-11); Pending referral to Senate Committee
|
|
HB 309
|
LAW CHANGES-COUNTY BUDGET COMMISSIONS (THOMAS D) To modify the law governing county budget commissions and property taxation.
|
12/19/2025 – Signed by Governor, effective 3/20/26.
|
|
HB 335
|
LIMIT INSIDE MILLAGE REVENUE INCREASES – (Thomas) To limit revenue increases from inside millage levies occurring due to a reappraisal or update, to allow a reduction of inside millage to accompany a school district income tax levy, to allow a reduction of inside millage to accompany a municipal income tax levy, and to require county budget commission approval of inside millage reductions to accompany a county sales tax levy.
*Monitoring for impact on local human services levies
*Governor has established Task Force to study property tax reform and submit report
*LSC Analysis and *Comp Doc analysis |
12/19/2025 – Signed by Governor, effective 3/20/26
|
|
HB 346
|
CHILD ABUSE MANDATORY REPORTING (KISHMAN M, WILLIAMS J) To require mandatory reporters of child abuse or neglect to report to both a peace officer and the public children services agency.
*Working with other stakeholders to express concerns about duplication and educating lawmakers on reporting process.
|
11/12/2025 - House Public Safety, (Second Hearing)
|
|
HB 393
|
COMMUNITY CORRECTIONS-OBTAINING ID CARDS (CLICK G, BREWER D) To require that community-based correctional facilities and programs assist inmates in obtaining state identification cards prior to release.
|
11/19/2025 – Passed by House (89-0); 3/24/26 --Reported out of Senate Community Revitalization Committee
|
|
HB 453
|
REQUIRE MEDICAID COVERAGE AND PAYMENT FOR ABA THERAPY (Lorenz)
- Requires third-party payers to reimburse applied behavior analysis service providers for performing ABA and treatment procedures at a minimum of 100% of the Medicaid fee schedule.
|
2/17/26 – House Insurance Committee (2nd Hearing)
|
|
HB 508
(Support)
|
LAW CHANGES-APRN PRACTICE (GROSS J, BAKER R) To modify the laws governing the practice of advanced practice registered nurses and to name this act the Better Access to Health Care Act.
- Grants an APRN the option to practice without a
- standard care arrangement and collaborating practitioner if the APRN has practiced in a clinical setting for 5,000 hours.
- Submitted proponent testimony
|
3/17/26 - House Medicaid, (Fourth Hearing)
|
|
HB 515
|
ADAMH BOARD COMPOSITIONS, CONTRACTS (WILLIAMS J) Regarding the composition of boards of alcohol, drug addiction, and mental health services and regarding board contracts.
- Requires political affiliation to be considered for Board appointment;
- Includes new language regarding a Boards’ contracting authority: “No board shall deny a contract to or refuse to contract with a for-profit entity or nonprofit entity, including a faith-based entity, based solely on the entity's for-profit or nonprofit status.”
|
10/15/2025 – Referred Committee House Children and Human Services
|
|
HB 579
|
REGULATE AI USE-HEALTH INSURERS (SCHMIDT J) To regulate the use of artificial intelligence by health insurers.
|
3/17/2026 - House Insurance, (First Hearing)
|
|
HB 709
|
MENTAL TELEHEATH COVERAGE REQUIREMENTS (BROWNLEE K, CRAIG M) To require private insurers to cover telehealth services for mental health services the same as for in-person mental health services.
|
2/25/2026 - Referred to Committee House Insurance
|
|
HB 716
*Support
|
CREATE ALL-PAYER CLAIMS DATABASE (CRAIG M, DEETER K) To create within the Department of Insurance an all-payer claims database.
|
3/17/2026 - House Insurance, (First Hearing)
|
|
HB 718
*Support
|
BEHAVIORAL HEALTH PROFESSIONALS REGULATION (BROWNLEE K, SALVO J) To change the name of the Chemical Dependency Professionals Board to the Behavioral Health Professionals Board, to require the Board to certify peer supporters and qualified mental health professionals, and to make other changes to the laws governing the Board and the professionals it regulates.
*Teresa testified in support along with a host of other stakeholders.
|
3/24/2026 - House Community Revitalization, (Second Hearing)
|
|
HB 724
*Support
|
HEALTH PLAN COVERAGE-BEHAVIORAL WELLNESS (SALVO J, WHITE A) To require a health benefit plan to provide coverage for annual behavioral health well checks.
|
3/4/2026 - Referred to Committee House Insurance
|
|
HB 742
|
REGARDING BEHAVIORAL HEALTH SCREENINGS (BAKER R, SALVO J) Regarding behavioral health screenings in the perinatal period and to make an appropriation
|
3/18/2026 - Referred to Committee House Children and Human Services
|
|
HB 780
|
ELIMINATE MEDICAID CARE MANAGEMENT SYSTEM (BROWNLEE K) To eliminate the care management system from the Medicaid program and to name this act the Medicaid Savings Act. (Similar to companion bill in the Senate – SB 386)
|
3/25/2026 - Referred to Committee House Medicaid
|
|
SB 1
|
ADVANCE OHIO HIGHER EDUCATION ACT (CIRINO J) To enact the Advance Ohio Higher Education Act regarding the operation of state institutions of higher education
- Similar to SB 83 from last GA (Companion to HB 6)
Allows waiver for professional licensure requirements for social work; counseling; and other healthcare classes.
|
3/28/25 – Enacted.
Signed by Governor DeWine. Effective June 30, 2025
|
|
SB 7
(Support)
|
REGARDING INSTRUCTION-SUBSTANCE USE (JOHNSON T) Regarding instruction for public and chartered nonpublic school students in the harmful effects of substance use.
- Reaching out to sponsor to discuss prevention generally and express support; Senator Johnson is also sponsor of SB 105 (ADAMHS board bill) from last GA
|
4/30/2025 – Passed by the Senate; 9/30/25 – First Hearing in House Ed Committee
|
|
SB 56
*Vehicle used to consolidate marijuana rules along with Intoxicating Hemp regulations
|
LAW CHANGES-MARIJUANA, LIQUOR, HEMP – (Huffman) To revise specified provisions of the liquor control, hemp, and adult-use marijuana laws, to levy taxes on certain hemp products, and to make an appropriation.
*10% tax on marijuana sales; distributes revenue to (36%) to local governments and remaining (64%) to state GRF
*Modifies regulations of Intoxicating Hemp products, including THC beverages to be compliant with new federal rules.
*See LSC Summary of Conference Committee Report
|
12/19/25 – signed by Governor, effective immediately.
*Referendum effort failed and thus, will not be on the ballot in November.
|
|
SB 138
(Support)
|
MODIFY ADAMH SERVICES LAWS (JOHNSON T) To modify various laws regarding boards of alcohol, drug addiction, and mental health services and to impose penalties for not registering recovery housing residences.
- Compromise language approved by the OC Board
- OC, OACBHA and OARP support
- Added criminal penalties for recovery residence violations
- Resource materials and training being developed jointly by OC and OACBHA.
|
7/1/25 – Signed by Governor; effective 9/30/25.
|
|
SB 160
|
REGARDING PRESCRIPTION DRUGS-MEDICATION SWITCHING (LISTON B, JOHNSON T) Regarding prescription drugs and medication switching.
- Prohibits insurers from making mid-year drug formulary changes that disrupt physician’s ability to exercise medical expertise to help their patients.
|
10/21/2025 -- Senate Financial Institutions and Insurance (third hearing.
|
|
SB 162
|
REGARDING HEALTH INSURANCE RECOUPMENT (BLESSING III L) Regarding the timeframe for health insurer recoupment from health care providers.
- Changes 24-month takeback timeframe, decreasing it to the same timeframe given to a provider to submit a claim, and also prohibit insurers from changing these timeframes during a contract period.
- Would prohibit insurers from charging a provider for appealing a determination of overpayment.
|
3/25/26 - Senate Financial Institutions and Insurance (3rd Hearing) Sub bill accepted
|
|
SB 164
|
REGULATE ARTIFICIAL INTELLIGENCE-HEALTH INSURERS (CUTRONA A) Regulate the use of artificial intelligence by health insurers.
- Requires transparency by insurers on the use of AI tools in prior authorization determinations and ensures that determinations are made through review of individual merits of claims by licensed clinical professionals.
|
10/28/2025 – First hearing Senate Financial Institutions and Insurance
|
|
SB 165
|
PROHIBIT HEALTH INSURERS-CERTAIN CLAIM DENIALS (MANCHESTER S) To prohibit a health insuring corporation from reducing or denying a claim based on certain factors.
- Contains prohibitions on down-coding for all providers, including prohibitions on limitations on reimbursement for time spent with patients.
|
10/14/2025 - Senate Financial Institutions and Insurance (First hearing
|
|
SB 166
|
PROHIBIT FEES-HEALTH INSURER, MEDICAID ELECTRONIC CLAIMS (MANNING N) To prohibit fees for electronic claims submission by health insurer and the Medicaid program.
- Would prohibit insurers from imposing a charge or fee, (including through withholding from payment), on any provider for electronic fund transfers or remittance advice transactions.
|
4/2/2025 - Referred to Committee Senate Medicaid
|
|
SB 197
|
VARIOUS CHANGES-INTERNET GAMBLING (MANNING N) To legalize internet gambling and levy a tax on businesses that provide internet gambling, to permit internet lottery gaming and online wagering on horse racing.
- Authorizes three new types of online gambling: internet gambling, lottery gaming, and online horse racing.
- Consolidates the regulation of gambling in Ohio under the authority of the Ohio Casino Control
- These provisions were not included in the budget bill
|
5/28/2025 - Senate Select Committee on Gaming, (Third Hearing)
|
|
SB 258
(Support)
|
BETTER ACCESS TO HEALTH CARE ACT (LANG G, ROMANCHUK M) To modify the laws governing the practice of advanced practice registered nurses
*Companion bill to HB 508
*Requires 2000 hours of practice in a clinical setting to practice without a SCA (most likely gets amended to 5000 hours)
*Sen. Romanchuk stated that bill is pending action on HB 508.
|
10/1/2025 - Referred to Committee Senate Health
|
|
SB 274
(Oppose)
Had positive discussion with Sen. Brenner. Bill not on fast-track. IP meetings expected
|
PROHIBIT MENTAL HEALTH SERVICES WITHOUT PARENTAL CONSENT (CIRINO J, BRENNER A) To prohibit the provision of mental health services to minors without parental consent.
*Companion bill to HB 172
*Removes 5122.04
|
10/1/2025 - Referred to Committee Senate Health
|
|
SB 276
|
INTERSTATE COMPACT-SCHOOL PSYCHOLOGISTS (ROEGNER K) To ratify the Interstate Compact for School Psychologists.
|
11/12/2025 – Passed Senate; 3/24/26 – House Education (1st hearing.)
|
|
SB 295
|
RESTORATION OF COMPETENCY-CRIMINAL(MANNING N, PATTON T) Relative to the timeline for restoration of competency in criminal cases and to declare an emergency.
- Increases the time during which a criminal defendant may be held for purposes of restoring the defendant’s competency – up to 3 years in some instances;
- Tolls or restarts the time limit for restoration of competency under certain circumstances.
- Retroactive to any criminal defendant found incompetent to stand trial prior to the effective date of the bill and whose restoration to competency is ongoing or whose case remains pending.
|
11/12/25 – Passed Senate (31-0); Passed House 2/19/26; Signed by Governor 2/20/26; eff. 2/20/26
|
|
SB 352
|
REGARDING BEHAVIORAL HEALTH SCREENINGS-PERINATAL PERIOD (WEINSTEIN C, TIMKEN J) Regarding behavioral health screenings in the perinatal period and to make an appropriation.
*Companion to HB 742
|
3/3/2026 - Senate Finance, (First Hearing)
|
|
SB 386
|
ELIMINATE CARE MANAGEMENT SYSTEM-MEDICAID PROGRAM (BLESSING III L, LISTON B) To eliminate the care management system from the Medicaid program and to name this act the Medicaid Savings Act.
*Companion to HB 780
|
3/25/2026 - Referred to Committee Senate Medicaid
|
|
|
Ohio AG Releases 2026 Sunshine Laws Update
The Ohio Attorney General Dave Yost released the 2026 edition of the Ohio Sunshine Laws manual, which clarifies that messaging applications and platforms that automatically delete records should not be used to conduct public business.
The Sunshine Laws manual, affectionately called the “Yellow Book,” is issued annually during the national observance of Sunshine Week (March 15-21 this year). The manual is a guide to Ohio’s Public Records and Open Meetings laws and aims to help citizens and public servants understand their rights and responsibilities under the law.
In the 2026 edition, the “practical pointers” for records management include this new directive: “Avoid using platforms or applications that automatically delete records.” Applications used to exchange digital communications – texts, images or videos – that automatically disappear from the recipient’s device and servers after a set time or upon being viewed should not be used for public business. Common examples of these applications include Signal, WhatsApp and Snapchat.
Under Ohio law, whether something is public record depends on its content, not the platform used to send it. Automatically deleting communications before they can be reviewed or retained could violate the Public Records Act, the manual says, which is why such transient-messaging apps should not be used to conduct public business.
In the Yellow Book’s introduction, Yost invokes a recent Ohio case to underscore why transparency is essential. Ohio v. Wade Steen, et al involved two members of the State Teachers Retirement System who conspired about a $65 billion investment through secret communications outside of normal public board rules. In February, a judge ruled that the two had violated their fiduciary duties. Both were prohibited from serving on the STRS board in the future.
In addition to publishing the manual, the Public Records Unit of Yost’s office also offers free Sunshine Laws training, as does the Ohio Auditor of State’s Office. In Ohio, public officials (or a designated representative) must take this training at least once per elected term. The sessions are also open to the public. |
|
SB 56 Banning THC & CBD Products Goes into Effect
Ohio Senate Bill (SB) 56 has now taken effect, including new criminal charges, along with the state’s new intoxicating hemp ban, which includes THC and CBD beverages. SB 56 originally did have a THC-infused beverage provision in the bill that would have allowed for 5mg THC beverages until the end of December, but Ohio Governor Mike DeWine line-item vetoed that provision when he signed the bill into law in December.
An effort was made by a group called “Ohioans for Cannabis Choice” to place a referendum on the November ballot that would block the law, however that effort failed to certify enough signatures to be eligible for the ballot. In addition to banning THC beverages and hemp products, Ohio’s new law will:
- Reduce THC levels in marijuana extracts from 90% to 70%.
- Limit THC levels in adult-use flower to 35%.
- Prohibit smoking in most public places.
- Prohibit marijuana possession in anything outside of its original packaging.
- Criminalize bringing legal marijuana from another state back to Ohio.
- Require drivers to store marijuana in the trunk of their car while driving.
Proponents of SB 56 cite recent federal legislation that was passed in November, which bans products that contain 0.4mg of total THC per container. The federal ban, however, included a one-year implementation delay to allow states to create their own regulatory framework for the changes.
The fight to restore adult-use THC options is likely to continue. As such, the Ohio Council will continue monitoring any changes related to these laws and will keep Ohio Council members informed. |
|
HB 730 Could Leave Urban Areas with Huge SNAP Gaps
According to recent reporting by The Ohio Capital Journal, a recent bill put forward by the Ohio General Assembly, Ohio House Bill (HB) 730, restored 59 Ohio Counties’ Supplemental Nutrition Assistance Program (SNAP) shortfalls but left multi-million dollar gaps for several counties in urban areas.
Recent changes in the “One Big Beautiful Bill Act” has left Ohio with an estimated $38 million deficit for SNAP. HB 730 would restore $12.5 million to the program, but critics indicate that its distribution formula is not equitable based on need. The bill would split the $12.5M equally across all of Ohio’s 88 counties. Once a county is made whole, they would not get any additional funding, and then the remaining funds would be distributed equally until the funding is depleted.
Under this plan, the largest amount any county will receive is approximately $250,000. For this amount of funding, 59 Ohio counties will be made completely whole. It leaves, however, huge deficits in urban areas, including an estimated $7.5 million in Cuyahoga County, $5.6 million in Franklin County, and more than $2 million each in Hamilton, Lucas, and Montgomery counties.
Last Year, the “One Big Beautiful Bill Act” changed the distribution of administrative costs that the federal government would cover, which previously was reimbursed 50%, and will now require states to cover 75% of the administrative costs, with the federal government only contributing to 25%. Additionally, the bill added new error rate penalties, where based on a state’s SNAP error rate, it could be liable to cover 5-15% of its benefit costs. Researchers at Georgetown University estimate those changes together will increase Ohio’s SNAP contribution by 268%
In the most recent year on record, only eight states and the U.S. Virgin Islands had error rates low enough to avoid added costs. Ohio’s error rate was 9%, meaning the state would have to cover a tenth of its SNAP benefits, in addition to the new added administrative cost. The added administrative costs take effect this October, while the benefit share is set to begin in 2027.
The Ohio Council will continue to monitor these issues and will keep members informed. |
|
DBH Seeking Feedback in Crisis Services Survey
The Ohio Department of Behavioral Health (DBH) is seeking feedback from providers on the behavioral health crisis system to better understand how crisis services are currently delivered across Ohio and to identify existing challenges. Milliman is assisting DBH in managing the survey process, which includes overseeing the survey link, collecting responses, and synthesizing feedback. Your honest feedback is critical and will be used to help DBH and its partners enhance the support, resources, and effectiveness of Ohio’s behavioral health crisis system.
Your participation is greatly appreciated and will directly contribute to improvements in behavioral health crisis care and supports across Ohio. Thank you for your dedication and for helping to strengthen Ohio’s crisis system for individuals and families statewide. |
|
MSY Program Update: Temporary Pause on New Applications
The Ohio Department of Medicaid (ODM) recently announced a temporary pause on new applications for Multi-System Youth (MSY) funding, effective March 23, 2026. The pause reflects current spending levels and is intended to maintain services for youth already approved through the program through June 30, 2026.
MSY is part of the State MSY Program, a cross-system initiative supported through the Ohio Family and Children First Cabinet Council and implemented in partnership with multiple state agencies, including the Departments of Behavioral Health, Children and Youth, Developmental Disabilities, Education and Workforce, Medicaid, and Youth Services. The program is designed to supplement local resources and coordinate planning when other funding sources have been exhausted. While Care Management Entities (CMEs) may support application and coordination processes, the State MSY Program is not administered as part of the OhioRISE benefit.
The current pause reflects the status of available funding within the program and the need to sustain services for youth who have already been approved. As this information is shared more broadly, it will be important to continue grounding MSY within the State MSY Program and its intended role across systems.
Looking ahead, the state has indicated that updates to the program are expected in the coming months to provide greater clarity on program goals, expectations, and overall structure, as well as to support the long-term sustainability of these resources. The Ohio Council will continue to engage with state partners and stakeholders and will share additional information as it becomes available. |
|
OhioRISE Eligibility and Enrollment Update effective July 1, 2026
The Ohio Department of Medicaid (ODM) proposed changes to amend the OhioRISE: Eligibility and Enrollment Rule, 5160-59-02, so that enrollment in OhioRISE will become effective on the first day of the calendar month of eligibility. This change aims to align with the managed care program enrollment and reduce manual retro‑enrollments caused by inpatient behavioral health admissions.
The rule is intended to take effect on July 1, 2026. The Ohio Council submitted comments on this proposed rule change, encouraging ODM to clarify the expectation and payment responsibility, recoupment, and billing expectation for behavioral health services delivered earlier in the same calendar month before OhioRISE eligibility is determined, including expectations for cross-payer reconciliation when eligibility timing differs across state and managed care plan systems.
Clarification of financial responsibility for behavioral health services provided to children and youth is found in the OhioRISE Mixed Services Protocol. Managed care plans are still expected to handle the Child and Adolescent Needs and Strengths (CANS) assessments completed before OhioRISE enrollment. The Protocol will be updated as needed to support the rule change. |
|
Prevention Services Rule (5122-29-20) Proposed Revisions
The Ohio Department of Behavioral Health (DBH) has released a proposal to rescind and replace the Prevention Services rule (5122-29-20). Rather than eliminating the rule, this proposal would remove the current version and replace it with revised language that continues to address prevention services within the Administrative Code.
The current prevention services rule creates an uneven regulatory environment in that it exempts certain entities (i.e., health departments, schools, FCFCs, and certain faith-based entities) from certification requirements, while community mental health and community substance use disorder providers are required to meet certification and accreditation standards to provide and be paid for prevention services. The current rule includes language requiring coalitions to become certified in order to provider prevention services.
The proposed rule continues to regulate prevention services as a certifiable service and maintains exemptions from certification for certain entities, including expanding exemptions to include prevention coalitions.
The Ohio Council has consistently raised concerns with this structure, as it creates different regulatory expectations for providers delivering prevention services and does not establish a clear and consistent framework across the system.
A public hearing on the prevention rule will be held April 20, and written comments are due by 5:00 p.m. that same day. The Ohio Council is currently reviewing the proposal to prepare comments and will share those with Ohio Council members as they are available. |
|
DBH Proposed Rules OAC 5122-25 through 28
The Ohio Department of Behavioral Health (DBH) has released proposed changes to Ohio Administrative Code (OAC) chapters 5122-25 through 5122-28. These rules pertain to certification procedures for community behavioral health service providers, and this update is related to the department’s required 5-year rule review process.
After multiple public comment periods, the rules have been revised by DBH and reviewed by the Common Sense Initiative (CSI) office. Having received approval from CSI, DBH has proceeded with the original filing to JCARR.
The Ohio Council originally submitted comments on March 8, 2024 offering recommendations for improvements on the draft rule package. Those comments focused on a proposed QBHS position, expanded incident reporting requirements, and the national accreditation/deemed status implementation process. DBH revised the rule package and opened a second round of comments in October 2024, for which the Ohio Council submitted comments on October 29, 2024. Subsequently, the Ohio Council met with DBH legal and licensure and certification teams regarding our comments. We are currently in the process of reviewing this latest update to the draft certification rule to determine whether or not changes have been made that would remedy those concerns.
The Ohio Council will continue monitoring progress on these rules and will share comments as well as information for advocacy opportunities will Ohio Council members. Of note, DBH will hold a public hearing at 10 am on Friday, April 17, 2026, in the Lobby Hearing Room located on the ground floor of the Rhodes State Office Tower, 30 E. Broad Street, Columbus, Ohio. They will accept written and verbal testimony on the rules under consideration.
To Testify In-Person: THE PROCESS HAS CHANGED. If you want to testify in-person, send an email to [email protected] at least five (5) days prior to the hearing and indicate in the subject matter line “Attendance at CBHS Rules Hearing”. DBH requests that if you plan to give verbal testimony, please also have a written copy of your testimony to provide to staff, and to arrive at least 20 minutes before the hearing time.
To Submit Written Testimony: Please submit written testimony via email to [email protected] no later than 5pm on the day of the hearing. DBH asks that you please specify “Comments on CBHS Rules” in the subject line. Written testimony can also be mailed to Ohio Department of Behavioral Health, Attn: Lisa Musielewicz, 30 E. Broad St. Floor 36, Columbus, OH 43215. |
|
Register For the ODM Provider Webinar About the Next Generation MyCare Program!
As part of ODM’s effort to prepare providers for the Next Generation MyCare program, they are hosting a series of webinars. These webinars will share information about the program, what it means for you, and steps you may need to take ahead of the program roll out. ODM encourages providers in Phase 2 counties to join.
Webinars are held on the third Wednesday of each month from March through August, alternating between a session specific to the Ohio Department of Aging (AGE) providers and all other provider types. Register below for the session that best fits your needs and schedule. To learn more, visit the Next Generation MyCare Resources for Providers webpage. Recordings for each session type will be available online after the first session.
|
Event Name
|
Event Date and Time
|
Link
|
|
Next Generation MyCare Webinar for the Ohio Department of Aging (AGE) Providers
|
Wednesday March 18, 2026
9 a.m. – 10 a.m.
|
Click here to register
|
|
Next Generation MyCare Webinar for Providers
|
Wednesday April 15, 2026
9 a.m. – 10 a.m.
|
Click here to register
|
|
Next Generation MyCare Webinar for the Ohio Department of Aging (AGE) Providers
|
Wednesday May 20, 2026
9 a.m. – 10 a.m.
|
Click here to register
|
|
Next Generation MyCare Webinar for Providers
|
Wednesday June 17, 2026
9 a.m. – 10 a.m.
|
Click here to register
|
|
Next Generation MyCare Webinar for the Ohio Department of Aging (AGE) Providers
|
Wednesday July 15, 2026
9 a.m. – 10 a.m.
|
Click here to register
|
|
Next Generation MyCare Webinar for Providers
|
Wednesday August 19, 2026
9 a.m. – 10 a.m.
|
Click here to register
|
|
|
The Next Generation MyCare Program is Coming to You! Phase 2 Starts Next Month
Get ready – on April 1 the Ohio Department of Medicaid (ODM) is expanding its roll out of the Next Generation MyCare program. Phase 2 includes Sandusky, Erie, Henry, Williams, Defiance, Paulding, Fayette, Fairfield, Licking, and Ashtabula counties. As you prepare for the program, there are a few important things you need to know.
How to become a Next Generation MyCare provider
If you would like to provide services to Next Generation MyCare members, you must enroll with ODM and contract with the Next Generation MyCare plans. If you are already enrolled as an ODM provider and contracted with plans, no additional action is required. Ohio Department of Aging (AGE) enrolled providers can continue to deliver services and submit claims but must contract with the Next Generation MyCare plans if you have not already.
What if I am new to billing in the Next Generation MyCare program?
Billing services in the MyCare program are generally the same as the Next Generation Managed Care program. If you submit claims for Managed Care members today, consider using the same process for MyCare members. If you use a trading partner, contact them before the program starts to check if you need to take any extra steps for your claim to be accepted by ODM.
If you do not have an existing process in place today, consider which of the below options is best for you.
- Providers with a smaller volume of claims typically utilize the Direct Data Entry (DDE) process. DDE is when a provider submits a single claim to the Next Generation MyCare plan through their DDE portal. Learn how to enroll and submit claims via DDE by visiting the plan’s DDE portals:
- Providers with a large volume of claims typically contract with a trading partner to submit claims via the OMES one front door. This supports the provider with billing and reconciliation. View ODM’s Electronic Data Interchange (EDI) Authorized Trading Partners list to see the trading partners currently authorized to work ODM and providers. Providers who want to use a trading partner are encouraged to contact a few to find the one that best fits their needs.
- Note: To submit claims for Next Generation MyCare members, you must use the correct plan Receiver ID and payer ID for the program. Additionally, you must use the member’s Medicaid ID even if they have other ID numbers.
- Refer to the Companion Guides for more information.
Want to learn more or have questions about the program?
Check out the Provider Frequently Asked Questions (FAQ) or Resources for Providers Webpage to learn more about how the program impacts you. For questions about billing services in the program, contact ODM Integrated Helpdesk at 800-686-1516 or [email protected]. Representatives are available Monday through Friday, 8 a.m. – 4:30 p.m. Eastern Time. |
|
White House Releases AI Framework
On March 20th, the White House released a policy framework for artificial intelligence (AI). The framework does not specifically address AI as it connects to health care policy; but it does urge Congress to override state AI laws that impose “undue burdens” but “not preempt states from enforcing their own generally appliable laws protecting children.” The framework’s goal is to establish federal standards to solve the patchwork of state laws that some believe have “hindered AI innovation”.
The Ohio Council will continue to monitor developments as it relates to both the Trump Administration AI Framework as well as the TRUMP AMERICA AI Act for potential implications on healthcare policy and practice and will keep Ohio Council members informed of any developments. |
|
National Council Releases Guidance on Navigating Federal Grants Memorandum
As many will recall, on January 13 of this year, the Substance Abuse and Mental Health Services Administration (SAMHSA) terminated approximately 2,800 grants totaling roughly $2 billion, only to reverse course the following day following rapid advocacy efforts. While the immediate crisis was averted, the federal grants landscape remains uncertain, and it will be important to be prepared for any similar events in the future should they occur.
To help their members navigate this environment, National Council engaged Feldesman, LLP, their trusted outside counsel, to prepare a comprehensive guidance memorandum. They have prepared a summary of that memo, available to you here.
The summary covers four key areas:
- The "termination for convenience" provision and how it was used, and may be used again, to cancel grants with limited notice.
- Strategic planning guidance, including how to assess program vulnerability.
- The new three-day Congressional notification requirement included in the fiscal year 2026 appropriations bill, and the litigation and advocacy opportunities it creates.
- A proposed SAM.gov certification requirement related to diversity, equity, and inclusion restrictions that could, if finalized, apply universally across all federal grant awards regardless of issuing agency.
The National Council notes that this summary is not meant to constitute legal advice, but rather guidance based upon outside counsel’s analysis. They encourage providers to review this resource and to reach out if they have questions about any of the issues it raises. They can be reached via email at [email protected]. |
|
Senate Passes Bipartisan Housing Act
On March 12th, the Senate passed the “21st Century ROAD to Housing Act” (S.Amdt.4308), a unified, bipartisan housing supply package, by a vote of 89-10. The bill, led by Senate Banking Committee Chair Tim Scott (R-SC) and Ranking Member Elizabeth Warren (D-MA), includes most of the provisions from the Senate’s “ROAD to Housing Act” (S.2651), and six provisions from the House’s “Housing for the 21st Century Act” (H.R.6644). If enacted, it would be the largest bipartisan housing supply bill passed by Congress in decades.
Despite overwhelming bipartisan support in the Senate and the White House’s backing, the “21st Century ROAD to Housing Act” faces an uncertain future in the House. Donald Trump threatened on March 18th that he would not sign any bills into law until the “Safeguard American Voter Eligibility (SAVE) America Act” (H.R. 7296) is passed; and the House Financial Services Committee (HFSC) Chair French Hill (R-AR) said in an earlier statement that the Senate’s unified package does not sufficiently represent the interests of House Republicans. Any changes made in the House would require the bill to return to the Senate for another round of voting.
Key provisions of the bill include:
- The “Reforming Disaster Recovery Act,” which contains critical reforms proposed by NLIHC’s Disaster Housing Recovery, Research, and Resilience Coalition (DHRC) to help ensure the federal government’s long-term disaster recovery program, HUD’s Community Development Block Grant–Disaster Recovery (CDBG-DR) program, better serves disaster survivors and disaster-impacted communities with the lowest incomes.
- The “Rural Housing Service Reform Act,” which would help preserve affordable rental and homeownership opportunities for low-income people and families living in rural areas, cut red tape, and encourage public-private partnerships to increase investment in the country’s rural housing supply. Importantly, by decoupling rental assistance from maturing mortgages, the bill would help preserve affordable housing in rural areas and maintain housing access for 400,000 rural families.
- Two provisions from the “Choice in Affordable Housing Act” related to streamlining inspections for the Housing Choice Voucher (HCV) program to make it faster and easier for HCV recipients to access housing in communities of their choice.
- The “Incentivizing Local Solutions to Homelessness Act,” which would allow for greater flexibility in how communities can use Emergency Solutions Grant funding to address the needs of people experiencing unsheltered homelessness.
- The “Housing Unhoused Disabled Veterans Act,” which would help more veterans experiencing homelessness access housing opportunities through the HUD-Veteran Affairs Supportive Housing (HUD-VASH) program.
For those who are supportive of this legislation and interested in providing support, the National Low Income Housing Coalition has created a Take Action page to help you contact your members of Congress. |
|
Trump, CMS, & Congress to Increase Waste, Fraud, & Abuse Efforts
CONGRESSIONAL FWA INITIATIVES: On March 5, 2026, the U.S. House Committee on Energy and Commerce (ECC) announced that they were moving forward to intensify their investigations to address fraud, waste, and abuse (FWA) across Medicaid. The committee will be building on prior oversight activities to expand investigations nationwide.
The ECC also specifically cited reviews for suspected Medicaid fraud in 10 states: California, Colorado, Massachusetts, Maine, Nebraska, New York, Oregon, Pennsylvania, Vermont, and Washington, citing that “each of these states displayed concerning cases of Medicaid fraud over the last several years”.
These developments are generating significant concern among state Medicaid leaders, with the National Association of Medicaid Directors convening regular discussions in response. More broadly, the federal administration is expected to maintain a strong focus on identifying and reducing FWA in both Medicaid and Medicare, signaling increased scrutiny for providers over the next several years.
TRUMP ADMINISTRATION FWA INITIATIVES: Additionally, the Trump Administration continues to focus efforts on FWA in federal healthcare programs. The administration has announced several immediate actions, including a nationwide Medicare enrollment moratorium on certain Durable Medical Equipment, Prosthetics, Orthotics, and Supplies (DMEPOS) suppliers and the deferral of $259.5 million in federal Medical funding to Minnesota while they investigate claims for potential fraud.
CMS FWA INITIATIVES: Likewise, the Centers for Medicare & Medicaid Services announced a new fraud prevention program, the Comprehensive Regulations to Uncover Suspicious Healthcare (CRUSH) initiative. Federal officials say the broader CRUSH strategy is intended to prevent fraud before it occurs, hold bad actors accountable, and protect taxpayer dollars while improving affordability across federal health programs. The effort is intended to strengthen program integrity in Medicare and Medicaid by expanding fraud detection tools, increasing oversight of providers and suppliers, and engaging stakeholders to identify additional strategies to prevent improper billing and payments.
The Ohio Council will continue to monitor trends in FWA investigations and will keep members informed of potential implications to access to behavioral health services or opportunities for advocacy. |
|
Congressional Update
Congress returned to session this week after a brief “spring break” recess with several issues, priorities, and deadlines to navigate. While lawmakers and the Whitehouse continue negotiations on Department of Homeland Security (DHS) funding (the remaining FY 2026 appropriations bill), the FY 2027 funding process is underway. Even though the Trump Administration has not released its FY 2027 budget blueprint, federal lawmakers are beginning to examine agency budgets and review policies that are funded by the various appropriations measures. As you know, the FY 2026 funding expires on September 30 so there is considerable work to be done prior to the summer recess.
Additionally, House GOP leaders continue to contemplate another reconciliation bill; however, any proposed policies would need to follow the rules of reconciliation, and any new spending would have to be offset with cuts elsewhere. This conversation will likely pick up over the coming weeks. The Senate and House remain in gridlock over bipartisan housing affordability legislation, ROAD to Housing Act 2025, which may become a lengthier stalemate.
On March 17, the House Energy and Commerce Subcommittee on Oversight and Investigations held Protecting Patients and Safeguarding Taxpayer Dollars: The Role of CMS in Combating Medicare and Medicaid Fraud. The hearing examined the Centers for Medicare & Medicaid Services’ (CMS) actions to address fraud across Medicare and Medicaid; the available authorities, tools and approaches for CMS to detect, prevent or remedy fraudulent claims and payments; and whether recent CMS enforcement actions are appropriately targeting fraud in these programs.
Aligning with these efforts, Trump has signed a new executive order (see the fact sheet) to launch a task force to eliminate fraud within federal benefit programs. The task force will advise the president and coordinate government-wide efforts to combat widespread fraud, waste and abuse in federal benefit programs, including housing, food, medical care and cash assistance administered with state and local partners. And on March 26, the Health Subcommittee held a hearing to examine policies that address the illicit drug threats in order to protect Americans families and keep communities safe.
The Ohio Council will continue to monitor all of the trends in federal oversight and will keep Ohio Council members informed of any potential policy changes or practice implications. |
|
Ohio's P.E.A.C.E. Behavioral Health On-line Training Now Available
The Center for Psychedelic Drug Research and Education (CPDRE) announced the launch of the Psychedelic Emergency, Acute, and Continuing care Education (P.E.A.C.E.) self-paced, on-line training program for Behavioral Health Professionals, developed by the CPDRE at The Ohio State University and supported through a grant from the Ohio Department of Behavioral Health. This fully online training is free to licensed behavioral health professionals in the state of Ohio and takes approximately 3.5 hours to complete. Those who complete all training requirements will receive a Certificate of Completion from the CPDRE.
In Ohio, an estimated 12,000 youth (ages 12–17) and 254,000 adults (18+) reported psychedelic use in the past year. These numbers are expected to rise, bringing a corresponding increase in psychedelic-related crisis encounters involving behavioral health responders.
This training is designed to equip behavioral health professionals and community responders with the knowledge, attitudes, and skills necessary to effectively recognize and respond to psychedelic-related crises. Participants will learn evidence-informed approaches that prioritize safety, de-escalation, and compassion while supporting improved outcomes for individuals in distress and those providing care. Through a trauma-informed and collaborative framework, the training explores strategies to reduce the risk of harm or escalation, strengthen coordination across medical, behavioral health, and public safety systems, and minimize liability for responders and organizations.
Click Center for Psychedelic Drug Research and Education to learn more about the training and to REGISTER HERE for free. |
|
Spring Gambling Disorder Training Series
The Problem Gambling Network of Ohio (PGNO) has announced training dates for it's three-part Spring Gambling Disorder Stages Training series. Completing all three courses provides the 30 hours needed to become qualified in treating gambling disorder through a Gambling endorsement for those licensed through the OCDP Board, or adding it to a clinician's scope of competency for those licensed through the CSWMFT board. Click the links below for more information and to register. Questions? Email [email protected].
April 1-3 | Stage I: Gambling, Problem Gambling, and Ohio's Service System
May 6-8 | Stage II: Applications and Approaches in Treating Problem Gambling Disorder
June 4-5 | Stage III: The Roles of Family and Finances in Treating Gambling Disorder |
|
OSPF Suicide Prevention Agency Training Series
Through a SAMHSA Garrett Lee Smith Youth Suicide Prevention Grant, The Ohio Suicide Prevention Foundation (OSPF) has the ability to provide free suicide prevention, screening, risk assessment, and treatment training at your facility, for your staff. Normally, these training courses can cost upwards of $100-$350+ per person.
OSPF has various training opportunities for both clinical staff (counselors, psychologists, social workers, physicians, etc.) and non-clinical staff (clerical staff, care coordinators, scheduling department, etc.). CEUs are provided for licensed social workers, counselors, and psychologists. Please see below for the types of trainings we can potentially provide at your facility, for your staff, free of charge.
Collaborative Assessment and Management of Suicidality (CAMS) training:
- CAMS is an evidenced-based treatment framework used to assess suicidality and specifically treat suicide risk. CAMS 3-part training provides mental health professionals (and other relevant professionals) with essential knowledge in using the CAMS framework to collaborate with patients in the treatment of their suicidal drivers.
- 7.0 CEs for Ohio Counselors, Social Workers, and Psychologists will be provided after completing the entire training
Assessing and Managing Suicide Risk (AMSR) training:
- Assessing and Managing Suicide Risk (AMSR?) for Health and Behavioral Health Professionals Working in Outpatient Settings (AMSR-Outpatient) formulation model and helps clinicians feel confident navigating challenging conversations about suicide. AMSR offers key strategies for providing compassionate care to people at risk for suicide.
- Participants who fully complete this training will also be eligible for 6.5 hours of continuing education credits from APA and NASW. As these are National-level CEs, you will need to check with your respective Ohio licensing board to see if they will accept your CEU certificate awarded after the training
If you are interested in discussing opportunities for free onsite training for your staff, please reach out to Austin Lucas at [email protected] with any questions. |
|
OCI February 2026 Edition
Federal Policy & Legislation
State Policy & Legislation
Reports & Resources
Training & Events
|
|
OCAM 2025 Prevention Education Series
The Ohio Coaching and Mentoring Network (OCAM) has released details on it's free, eight-part 2025 Prevention Education Series for new prevention professionals.
This training series is designed for participants who have less than one year in prevention and who have already gained the Registered Applicant status. Participants are expected to attend all sessions and will receive 24 CEUs to be used toward an OCPSA credential. Topics include:
- Hidden Dangers of Over-the-Counter Medications
- Healthy Relationship Approaches
- Grant Writing
- Ethical Decision-Making in Prevention
- Prevention Science Foundations
- Prevention Supervision
- Coalition Building
View the complete training schedule and registration information here. |
|
RFA Due Mar 6th: Expansion of Peer Run Orgs & Clubhouses
The Ohio Department of Behavioral Health (DBH) Bureau of Recovery Supports has released a Request for Applications (RFA) for the purpose of soliciting applications from eligible applicants for expansion of services of existing certified peer-run organizations (up to $65,000), and the creation of new certified peer-run organizations (up to $160,000).
This RFA seeks to select multiple grantees. The responsibilities of the selected applicants will include expansion of services, or the creation of a new peer-run organization, as outlined in the Scope of Work. DBH will award funding only to qualified organizations that provide services as outlined in the Scope of Work. The responsibilities of the selected applicants will include expansion of services, or the creation of a new peer-run organization, as outlined in the Scope of Work. DBH will award funding only to qualified organizations that provide services as outlined in the Scope of Work.
An accredited Clubhouse is a community-based mental health recovery center that has been certified for its high-quality adherence to the "International Standards for Clubhouse Programs." Unlike more traditional clinical settings, Clubhouses operate as a community where individuals living with mental illness work side-by-side and partner with staff to run the organization. Here’s a brief video to highlight the work of Clubhouses and the expansion effort in Ohio: Clubhouse Ohio video (5 minutes)
Applications must be emailed to [email protected] by 3:00 p.m. on March 6. Awards are expected to be announced the week of March 27.
View the full RFA here. |
|
Suicide Screening & Assessment Fact Sheet
The Suicide Prevention Resource Center recently released a new fact sheet, Suicide Screening and Assessment, which outlines two core approaches to identifying suicide risk and clarifies how they function within a comprehensive prevention framework. Rather than defining these practices at a basic level, the resource focuses on how screening tools and clinical assessments operate together—screening serving as an initial risk flag and assessment providing the deeper clinical evaluation needed to determine acuity, safety needs, and care pathways.
The fact sheet underscores that neither approach is sufficient in isolation. Their effectiveness depends on strong implementation infrastructure, including trained staff, clear clinical protocols, collaborative safety planning, and warm handoffs to treatment and crisis supports. While predictive limitations of risk tools remain, the field consensus continues to support standardized screening paired with comprehensive follow-up as a core component of suicide prevention systems across behavioral health, healthcare, and community settings. |
|
Supportive Housing Transitions & Racial Disparities Studies
The National Alliance to End Homelessness has released two new studies, “Leaving Permanent Supportive Housing When Clients Are Ready: How Providers Can Help” and “When Housing Homeless Older Adults, Race Matters,” as part of its Research into Action initiative, which translates research into practical guidance for homelessness response systems. Together the reports examine how housing interventions shape long-term stability, with one focusing on transitions out of Permanent Supportive Housing (PSH) and the other analyzing racial and age disparities in housing outcomes among older adults.
Leaving Permanent Supportive Housing: When Clients are Ready: How Providers Can Help, explores what predicts successful exits from PSH and how providers can support tenants who wish to move into more independent housing. While PSH is designed as long-term housing paired with supportive services, the study finds that some tenants voluntarily leave for other permanent housing arrangements and often do so successfully. A large majority of individuals who exited PSH for permanent housing without ongoing services did not return to homelessness. The research also found that longer stays in PSH were associated with stronger exit outcomes, suggesting that sustained stability, income growth, and service engagement help prepare tenants for independent housing.
The study further identifies factors that influence successful transitions. Individual characteristics, such as age, race, gender, and behavioral health history, intersect with community and program conditions. Housing market affordability plays a major role in whether tenants can successfully move on, while program features like staffing levels, funding structures, and turnover rates also shape outcomes. To support providers and tenants, researchers developed a readiness assessment tool (Life After Supportive Housing – LASH), to guide collaborative transition planning, focusing on financial readiness, service connections, and tenant confidence. The report emphasizes that exits should always be tenant-driven and supportive with thoughtful planning rather than motivated by system pressure to create unit turnover.
The companion study, When Housing Homeless Older Adults, Race Matters, examines how race and age intersect to influence returns to homelessness. Using longitudinal homelessness data, the research finds that the risk of recurrent homelessness increases with age and is disproportionately higher for Black and American Indian/Alaska Native older adults compared to their White counterparts. However, placement into housing interventions—particularly Permanent Supportive Housing and Rapid Re-Housing—significantly reduces this risk across all populations and does so even more substantially for older adults of color. The study concludes that expanding access to these interventions, while addressing structural inequities in housing placement and service delivery, is critical to improving stability outcomes as the population of older adults experiencing homelessness continues to grow. |
|
BH Conditions Outrank Diabetes, Cancers Among Commercially Insured
A recent FAIR Health white paper, Chronic Conditions in the United States: A Study of Commercial Claims, found that chronic behavioral health conditions account for close to one-third of the most prevalent health matters among commercially insured patients. Anxiety disorders, mental illness and depressive disorders were the three most frequently observed across insurance claims in 2024 — surpassing obesity, diabetes, heart disease and a swath of other chronic diagnoses.
The analysis explored 2024 commercial insurance claims data to examine the prevalence, comorbidity patterns, and cost burden of 44 chronic conditions. Drawing from one of the nation’s largest private claims databases, the report finds that chronic conditions are widespread among commercially insured adults, with 57.5% of patients having at least one chronic condition and many experiencing multiple co-occurring diagnoses. Healthcare spending rises sharply with each additional condition, underscoring the compounding clinical and financial impact of chronic disease.
When examining the most prevalent chronic conditions in the commercially insured population, anxiety disorders (14.6%), depressive disorders (8.8%), and broader mental illness diagnoses (10.5%) rank among the most common overall. Collectively, chronic behavioral health conditions account for close to one-third of the most prevalent chronic health conditions identified in the study—placing them alongside cardiometabolic conditions like hypertension, obesity, and hyperlipidemia as major drivers of population health need.
The report also highlights the high comorbidity and cost implications associated with chronic conditions, including behavioral health. Many patients experience multiple overlapping diagnoses, which significantly increases service utilization and annual healthcare spending. These findings reinforce the role of behavioral health not as a siloed specialty issue but as a central component of chronic disease management—shaping overall health outcomes, cost trajectories, and care coordination needs across the commercially insured population. |
|
Mental Health Among Leading Causes of Employee Short-Term Disability Claims
A recent workforce absence trends brief from Sedgwick, “Looking Back to Look Forward: 2025 Workforce Absence Trends and 2026 Outlook,” has identified mental health conditions as one of the leading drivers of employee short-term disability claims.
While pregnancy remains the top cause of short-term disability among workers under age 45, mental health and substance use conditions are now close behind and rising across multiple age groups. For employees ages 35–44, mental health claims are nearly equivalent to pregnancy-related claims and are projected to surpass them. Increases are also evident among younger workers and those ages 55+, signaling a broadening workforce impact.
The brief underscores that traditional employer responses—such as referrals to Employee Assistance Programs alone—are no longer sufficient, particularly amid ongoing behavioral health workforce shortages. Employers are being pushed to adopt more comprehensive mental health strategies, including expanded accommodations, stigma reduction, holistic benefits, and integrated leave and disability supports. The report frames mental health not only as a clinical concern but as a central workforce and productivity issue that will continue shaping disability costs, benefit design, and organizational planning in the years ahead.
Read the full report here. |
|
Anxiety, Depression, & Barriers to Care for Clients with IDD
A recent study published in JAMA Network Open, “Anxiety, Depression, and Care Barriers in Adults with Intellectual and Developmental Disabilities,” examines national patterns in mental health prevalence, treatment use, and access barriers among adults with intellectual and developmental disabilities (IDDs). Using pooled 2021–2023 National Health Interview Survey data, researchers compared adults with IDDs to adults without functional limitations to better understand disparities in diagnosis, symptom burden, and service access.
Findings show markedly elevated mental health needs among adults with IDDs. More than half reported diagnoses of anxiety (57.2%) and depression (57.1%), rates nearly ten times higher than those observed among adults without disabilities. Daily anxiety and depression symptoms were also significantly more common, as was use of psychiatric medications and counseling services. Despite higher treatment engagement, adults with IDDs continued to experience more frequent and severe symptom presentations, underscoring persistent unmet clinical need.
The study also highlights structural barriers to care. Adults with IDDs were substantially more likely to delay or forgo counseling due to cost and faced broader access challenges tied to socioeconomic vulnerability, public insurance reliance, and service system limitations. Authors conclude that the findings point to the need for disability-informed mental health delivery models, expanded affordability, and workforce training to address the scale of disparity. Strengthening accessible, culturally and disability-responsive care systems will be critical to reducing inequities in mental health outcomes for this population. |
|
Integrating SUD Prevention with Physical Care
The Substance Abuse and Mental Health Services Administration (SAMHSA) Center for Financing Reform and Innovation (CFRI) has released a new report on Integrating Substance Use Disorder Prevention with Physical Health Care: Progress in States.
Over the past several decades, rising rates of substance misuse, substance use disorders (SUD), and related harms, including nonfatal and fatal overdoses, have placed a significant burden on individuals, communities, and the health care system. The report argues that prevention is essential to avoid this chronic disease, and to improve public health. Integrating SUD prevention with physical health care is an effective strategy.
The report and webinar examine current approaches to integrating prevention with physical health care at the state level including implementation, financing, partnerships, challenges, and support needs, particularly for adolescents, and where states are in the implementation of services.
View the full resource here. |
|
Ohio SUD Deflection Data Collection & Definitions Guidance
The Ohio Deflection Association, in partnership with the Northeast Ohio Medical University's Criminal Justice Coordinating Center of Excellence’s (CJCCOE) Substance Use Deflection Initiative, has released a new Deflection Data Collection and Definitions Guide.
“Deflection” aims to connect individuals experiencing addiction with treatment and recovery according to the individual’s needs and away from traditional avenues, such as emergency departments or the criminal justice system.
This guide will help deflection teams across Ohio operate under the same standardized definitions; providing concrete definitions and delivery criteria for standard deflection services, such as:
- Outreach
- Referrals
- Treatment Connection
- Follow-Up
- Point of Care Follow-Up
By standardizing terminology, it will ensure accurate data collection statewide and strengthen the measurement of outcomes, highlighting the impact of innovative deflection efforts in communities across Ohio.
Read the full guide here. |
|
HPIO “SNAP at a Glance: Key Changes from HR 1”
The Health Policy Institute of Ohio (HPIO) has released a new policy explainer titled “SNAP at a Glance: Key Changes from HR 1.”
The Supplemental Nutrition Assistance Program (SNAP) enables more than 1.4 million Ohioans to meet their basic food needs and supports local economies by generating up to $1.50 in economic activity for every $1 in benefits spent.
HR 1, the federal reconciliation bill also known as the “One Big Beautiful Bill Act,” which was enacted in July 2025, made substantial changes to SNAP that will affect eligibility for the program, as well as how the program is administered by Ohio and other states. Ohio’s share of SNAP costs is projected to rise 268%, from $146 million to nearly $540 million, due to provisions in HR 1 that shift more administrative and benefit costs onto states.
The explainer describes how HR 1’s SNAP eligibility restrictions and expanded work requirements are expected to negatively impact the ability of Ohioans to access healthy food. |
|
Ohio General Assembly
Lawmakers have fully returned to action for the 2026 legislative session. Both the Ohio House and Senate chambers are holding various committee hearings and voting on bills. They will most likely break for the month of April to engage in primary election campaign activities but return to legislative work in May and June when they will again break for the summer and early fall for the general election campaign. As far as priorities go, lawmakers are expected to work on producing a Capital Budget, passing a Corrections Budget to adjust spending and policy technicalities, reviewing additional property tax reforms, monitoring the Medicaid funding shortfall, and continuing to focus on fraud waste and abuse oversight activities. As this legislative session advances, the Ohio Council staff will continue to review and monitor legislative activity, engage lawmakers and key staff, and advocate with DeWine administration officials on policy issues that affect the community behavioral health system. Accordingly, below are legislative measures that we have identified for further review or advocacy, and implementation monitoring.
|
HB28
|
ELIMINATE REPLACEMENT PROPERTY TAX LEVY AUTHORITY (MATHEWS A, HALL T) To eliminate the authority to levy replacement property tax levies.
|
|
|
Current Status:
|
4/8/2025 - Senate Ways and Means, (First Hearing)
|
|
|
State Bill Page:
|
https://www.legislature.ohio.gov/legislation/legislation-summary?id=GA136-HB-28
|
|
HB57
|
OVERDOSE REVERSAL DRUGS, SCHOOL RELEASED TIME (JARRELLS D, WILLIAMS J) Regarding school policies on the administration of overdose reversal drugs and limits on student attendance in released time courses in religious instruction.
|
|
|
Current Status:
|
10/20/2025 - SIGNED BY GOVERNOR; eff. 90 days
|
|
|
State Bill Page:
|
https://www.legislature.ohio.gov/legislation/legislation-summary?id=GA136-HB-57
|
|
HB58
|
RECOVERY HOUSING, ADDICTION SERVICES (PIZZULLI J, JARRELLS D) To require state certification of recovery housing residences, to establish additional duties regarding services offered by community addiction services providers, and to create the Ohio Recovery Housing Task Force.
|
|
|
Current Status:
|
2/25/2026 - PASSED BY HOUSE; Vote 92-0
|
|
|
State Bill Page:
|
https://www.legislature.ohio.gov/legislation/legislation-summary?id=GA136-HB-58
|
|
HB144
|
COMMUNICATION DISABILITY DATABASE EXPANSIONS (CLICK G) To expand the communication disability database to include any person with a disability, to expand access to that database through countywide 9-1-1 systems, and to name this act "Keith's Law".
|
|
|
Current Status:
|
10/20/2025 - SIGNED BY GOVERNOR; eff. 90 days
|
|
|
State Bill Page:
|
https://www.legislature.ohio.gov/legislation/legislation-summary?id=GA136-HB-144
|
|
HB172
|
REQUIRE PARENTAL CONSENT-MINORS' MENTAL HEALTH SERVICE (NEWMAN J) To prohibit the provision of mental health services to minors without parental consent.
|
|
|
Current Status:
|
11/19/2025 - House Health, (Third Hearing)
|
|
|
State Bill Page:
|
https://www.legislature.ohio.gov/legislation/legislation-summary?id=GA136-HB-172
|
|
HB186
|
REDUCE SCHOOL DISTRICT PROPERTY TAXES (HOOPS J, THOMAS D) To authorize a reduction in school district property taxes affected by a millage floor that would limit increases in such taxes according to inflation, to modify the process for certifying property tax abstracts, and to make an appropriation.
|
|
|
Current Status:
|
12/19/2025 - SIGNED BY GOVERNOR; eff. immediately
|
|
|
State Bill Page:
|
https://www.legislature.ohio.gov/legislation/legislation-summary?id=GA136-HB-186
|
|
HB189
|
REGARDING SCHOOL BEHAVIORAL THREAT MANAGEMENT (HALL T, GHANBARI H) Regarding a statewide behavioral threat management operational process for public and chartered nonpublic schools.
|
|
|
Current Status:
|
2/4/2026 - House Education, (Second Hearing)
|
|
|
State Bill Page:
|
https://www.legislature.ohio.gov/legislation/legislation-summary?id=GA136-HB-189
|
|
HB190
|
PUBLIC SCHOOLS-GENDER PRONOUN USE (NEWMAN J, WILLIAMS J) To enact the Given Name Act regarding the use of gender pronouns in public schools.
|
|
|
Current Status:
|
4/29/2025 - House Education, (First Hearing)
|
|
|
State Bill Page:
|
https://www.legislature.ohio.gov/legislation/legislation-summary?id=GA136-HB-190
|
|
HB219
|
ESTABLISH INSURER NETWORK ADEQUACY STANDARDS (DEETER K) To establish network adequacy standards for health insurers.
|
|
|
Current Status:
|
10/7/2025 - BILL AMENDED, House Insurance, (Second Hearing)
|
|
|
State Bill Page:
|
https://www.legislature.ohio.gov/legislation/legislation-summary?id=GA136-HB-219
|
|
HB220
|
REGARDING PRIOR AUTHORIZATION REQUIREMENTS (WORKMAN H) Regarding health insurance and Medicaid program prior authorization requirements.
|
|
|
Current Status:
|
2/17/2026 - House Insurance, (Fourth Hearing)
|
|
|
State Bill Page:
|
https://www.legislature.ohio.gov/legislation/legislation-summary?id=GA136-HB-220
|
|
HB298
|
LEGALIZE, REGULATE INTERNET GAMBLING (STEWART B, JOHN M) To legalize and regulate internet gambling in this state, to levy a tax on businesses that provide internet gambling, and to prohibit online sweepstakes games.
|
|
|
Current Status:
|
6/3/2025 - House Finance, (Second Hearing)
|
|
|
State Bill Page:
|
https://www.legislature.ohio.gov/legislation/legislation-summary?id=GA136-HB-298
|
|
HB309
|
LAW CHANGES-COUNTY BUDGET COMMISSIONS (THOMAS D) To modify the law governing county budget commissions and property taxation.
|
|
|
Current Status:
|
12/19/2025 - SIGNED BY GOVERNOR; eff. 3/18/26
|
|
|
State Bill Page:
|
https://www.legislature.ohio.gov/legislation/legislation-summary?id=GA136-HB-309
|
|
HB324
|
PRESCRIPTION DRUG CONDITIONS-SEVERE ADVERSE EFFECTS (MATHEWS A, CRAIG M) To establish conditions on the prescribing of prescription drugs causing severe adverse effects and to name this act the Patient Protection Act.
|
|
|
Current Status:
|
2/11/2026 - Referred to Committee Senate Health
|
|
|
State Bill Page:
|
https://www.legislature.ohio.gov/legislation/legislation-summary?id=GA136-HB-324
|
|
HB335
|
LIMIT INSIDE MILLAGE REVENUE INCREASES (THOMAS D) To limit revenue increases from inside millage levies occurring due to a reappraisal or update.
|
|
|
Current Status:
|
12/19/2025 - SIGNED BY GOVERNOR; eff. 3/18/26
|
|
|
State Bill Page:
|
https://www.legislature.ohio.gov/legislation/legislation-summary?id=GA136-HB-335
|
|
HB346
|
CHILD ABUSE MANDATORY REPORTING (KISHMAN M, WILLIAMS J) To enact V.J.'s Law to require mandatory reporters of child abuse or neglect to report to both a peace officer and the public children services agency.
|
|
|
Current Status:
|
11/12/2025 - House Public Safety, (Second Hearing)
|
|
|
State Bill Page:
|
https://www.legislature.ohio.gov/legislation/legislation-summary?id=GA136-HB-346
|
|
HB393
|
COMMUNITY CORRECTIONS-OBTAINING ID CARDS (CLICK G, BREWER D) To require that community-based correctional facilities and programs assist inmates in obtaining state identification cards prior to release.
|
|
|
Current Status:
|
2/17/2026 - Senate Addiction and Community Revitalization, (First Hearing)
|
|
|
State Bill Page:
|
https://www.legislature.ohio.gov/legislation/legislation-summary?id=GA136-HB-393
|
|
HB453
|
REGARDING COVERAGE, PRACTICE-APPLIED BEHAVIOR ANALYSIS (LORENZ B) Regarding insurance and Medicaid coverage of applied behavior analysis therapy for autism treatment and to permit exam-eligible technicians to engage in the practice of applied behavior analysis.
|
|
|
Current Status:
|
2/17/2026 - House Insurance, (Second Hearing)
|
|
|
State Bill Page:
|
https://www.legislature.ohio.gov/legislation/legislation-summary?id=GA136-HB-453
|
|
HB508
|
LAW CHANGES-APRN PRACTICE (GROSS J, BAKER R) To modify the laws governing the practice of advanced practice registered nurses and to name this act the Better Access to Health Care Act.
|
|
|
Current Status:
|
11/18/2025 - House Medicaid, (Third Hearing)
|
|
|
State Bill Page:
|
https://www.legislature.ohio.gov/legislation/legislation-summary?id=GA136-HB-508
|
|
HB515
|
ADAMH BOARD COMPOSITIONS, CONTRACTS (WILLIAMS J) Regarding the composition of boards of alcohol, drug addiction, and mental health services and regarding board contracts.
|
|
|
Current Status:
|
10/15/2025 - Referred to Committee House Children and Human Services
|
|
|
State Bill Page:
|
https://www.legislature.ohio.gov/legislation/legislation-summary?id=GA136-HB-515
|
|
HB525
|
REGARDING AI-THERAPY (COCKLEY C, MATHEWS T) Regarding the use of artificial intelligence in therapy services.
|
|
|
Current Status:
|
10/22/2025 - Referred to Committee House Health
|
|
|
State Bill Page:
|
https://www.legislature.ohio.gov/legislation/legislation-summary?id=GA136-HB-525
|
|
HB579
|
REGULATE AI USE-HEALTH INSURERS (SCHMIDT J) To regulate the use of artificial intelligence by health insurers.
|
|
|
Current Status:
|
11/12/2025 - Referred to Committee House Insurance
|
|
|
State Bill Page:
|
https://www.legislature.ohio.gov/legislation/legislation-summary?id=GA136-HB-579
|
|
HB587
|
REGARDING KRATOM PRODUCT SALES (ODIOSO M, LORENZ B) Regarding sales of kratom products.
|
|
|
Current Status:
|
2/25/2026 - House Agriculture, (First Hearing)
|
|
|
State Bill Page:
|
https://www.legislature.ohio.gov/legislation/legislation-summary?id=GA136-HB-587
|
|
HB622
|
MENTAL HEALTH, SUBSTANCE ABUSE PILOT PROGRAM CREATION (WILLIAMS J, ROBB BLASDEL M) To enact the Mental Health and Community Wellness Act to amend the competency to stand trial law, to create the mental health and substance abuse community-based correctional facility pilot program, to require a prosecutor to file for civil confinement of a defendant who is found incompetent to stand trial and who is charged with a felony or a misdemeanor offense of violence, and to make an appropriation.
|
|
|
Current Status:
|
2/4/2026 - Referred to Committee House Judiciary
|
|
|
State Bill Page:
|
https://www.legislature.ohio.gov/legislation/legislation-summary?id=GA136-HB-622
|
|
HB675
|
ESTABLISH MEDICAID MCO PAYMENT PROGRAM (STEPHENS J, DEETER K) To establish a temporary program for hospital payments made by Medicaid managed care organizations and to name this act the Healthier Rural Hospitals Act.
|
|
|
Current Status:
|
2/18/2026 - Referred to Committee Senate Finance
|
|
|
State Bill Page:
|
https://www.legislature.ohio.gov/legislation/legislation-summary?id=GA136-HB-675
|
|
HB680
|
REGARDING SUBSTANCE USE, MENTAL HEALTH TREATMENT-DEFENDANTS (WILLIAMS J) Regarding substance use disorder and mental health treatment for criminal defendants.
|
|
|
Current Status:
|
2/24/2026 - House Community Revitalization, (First Hearing)
|
|
|
State Bill Page:
|
https://www.legislature.ohio.gov/legislation/legislation-summary?id=GA136-HB-680
|
|
HB693
|
AFFIRMATION PROTECTION-MINOR'S SEX (CLICK G, WILLIAMS J) To enact the Affirming Families First Act and protect the right to affirm a minor child's sex.
|
|
|
Current Status:
|
2/18/2026 - Referred to Committee House Judiciary
|
|
|
State Bill Page:
|
https://www.legislature.ohio.gov/legislation/legislation-summary?id=GA136-HB-693
|
|
HB709
|
MENTAL TELEHEATH COVERAGE REQUIREMENTS (BROWNLEE K, CRAIG M) To require private insurers to cover telehealth services for mental health services the same as for in-person mental health services.
|
|
|
Current Status:
|
2/25/2026 - Referred to Committee House Insurance
|
|
|
State Bill Page:
|
https://www.legislature.ohio.gov/legislation/legislation-summary?id=GA136-HB-709
|
|
HB716
|
CREATE ALL-PAYER CLAIMS DATABASE (CRAIG M, DEETER K) To create within the Department of Insurance an all-payer claims database.
|
|
|
Current Status:
|
2/24/2026 - Introduced
|
|
|
State Bill Page:
|
https://www.legislature.ohio.gov/legislation/legislation-summary?id=GA136-HB-716
|
|
HB718
|
BEHAVIORAL HEALTH PROFESSIONALS REGULATION (BROWNLEE K, SALVO J) To change the name of the Chemical Dependency Professionals Board to the Behavioral Health Professionals Board, to require the Board to certify peer supporters and qualified mental health professionals, and to make other changes to the laws governing the Board and the professionals it regulates.
|
|
|
Current Status:
|
2/25/2026 - Introduced
|
|
|
State Bill Page:
|
https://www.legislature.ohio.gov/legislation/legislation-summary?id=GA136-HB-718
|
|
SB7
|
REGARDING INSTRUCTION-SUBSTANCE USE (JOHNSON T) Regarding instruction for public and chartered nonpublic school students in the harmful effects of substance use.
|
|
|
Current Status:
|
9/30/2025 - House Education, (First Hearing)
|
|
|
State Bill Page:
|
https://www.legislature.ohio.gov/legislation/legislation-summary?id=GA136-SB-7
|
|
SB56
|
LAW CHANGES-MARIJUANA, LIQUOR, HEMP (HUFFMAN S) To revise specified provisions of the liquor control, hemp, and adult-use marijuana laws, and to make an appropriation, and to amend section 4506.01 of the Revised Code effective December 31, 2026, to revise the law governing commercial driver's licenses.
|
|
|
Current Status:
|
12/19/2025 - SIGNED BY GOVERNOR; eff. immediately
|
|
|
State Bill Page:
|
https://www.legislature.ohio.gov/legislation/legislation-summary?id=GA136-SB-56
|
|
SB137
|
REQUIRE HOSPITALS-PROVIDE OVERDOSE REVERSAL DRUGS (JOHNSON T) To require hospitals to provide overdose reversal drugs under certain circumstances.
|
|
|
Current Status:
|
2/25/2026 - PASSED BY HOUSE; Vote 80-11
|
|
|
State Bill Page:
|
https://www.legislature.ohio.gov/legislation/legislation-summary?id=GA136-SB-137
|
|
SB138
|
MODIFY ADAMH SERVICES LAWS (JOHNSON T) To modify various laws regarding boards of alcohol, drug addiction, and mental health services and to impose penalties for not registering recovery housing residences.
|
|
|
Current Status:
|
7/1/2025 - SIGNED BY GOVERNOR; eff. 9/30/25
|
|
|
State Bill Page:
|
https://www.legislature.ohio.gov/legislation/legislation-summary?id=GA136-SB-138
|
|
SB162
|
REGARDING HEALTH INSURANCE RECOUPMENT (BLESSING III L) Regarding the timeframe for health insurer recoupment from health care providers.
|
|
|
Current Status:
|
10/21/2025 - Senate Financial Institutions, Insurance and Technology, (Second Hearing)
|
|
|
State Bill Page:
|
https://www.legislature.ohio.gov/legislation/legislation-summary?id=GA136-SB-162
|
|
SB164
|
REGULATE ARTIFICIAL INTELLIGENCE-HEALTH INSURERS (CUTRONA A) Regulate the use of artificial intelligence by health insurers.
|
|
|
Current Status:
|
10/28/2025 - Senate Financial Institutions, Insurance and Technology, (First Hearing)
|
|
|
State Bill Page:
|
https://www.legislature.ohio.gov/legislation/legislation-summary?id=GA136-SB-164
|
|
SB165
|
PROHIBIT HEALTH INSURERS-CERTAIN CLAIM DENIALS (MANCHESTER S) To prohibit a health insuring corporation or sickness and accident insurer from reducing or denying a claim based on certain factors.
|
|
|
Current Status:
|
10/14/2025 - Senate Financial Institutions, Insurance and Technology, (First Hearing)
|
|
|
State Bill Page:
|
https://www.legislature.ohio.gov/legislation/legislation-summary?id=GA136-SB-165
|
|
SB166
|
PROHIBIT FEES-HEALTH INSURER, MEDICAID ELECTRONIC CLAIMS (MANNING N) To prohibit fees for electronic claims submission by health insurer and the Medicaid program.
|
|
|
Current Status:
|
4/2/2025 - Referred to Committee Senate Medicaid
|
|
|
State Bill Page:
|
https://www.legislature.ohio.gov/legislation/legislation-summary?id=GA136-SB-166
|
|
SB197
|
VARIOUS CHANGES-INTERNET GAMBLING (MANNING N) To legalize internet gambling and levy a tax on businesses that provide internet gambling, to permit internet lottery gaming and online wagering on horse racing, to make other changes to the Gambling Law, and to make an appropriation.
|
|
|
Current Status:
|
5/28/2025 - Senate Select Committee on Gaming, (Third Hearing)
|
|
|
State Bill Page:
|
https://www.legislature.ohio.gov/legislation/legislation-summary?id=GA136-SB-197
|
|
SB207
|
PROHIBIT COST SHARING PRACTICES-CERTAIN HEALTH INSURANCE (MANCHESTER S, LISTON B) To prohibit certain health insurance cost-sharing practices.
|
|
|
Current Status:
|
11/4/2025 - Senate Financial Institutions, Insurance and Technology, (Third Hearing)
|
|
|
State Bill Page:
|
https://www.legislature.ohio.gov/legislation/legislation-summary?id=GA136-SB-207
|
|
SB258
|
BETTER ACCESS TO HEALTH CARE ACT (LANG G, ROMANCHUK M) To modify the laws governing the practice of advanced practice registered nurses and to name this act the Better Access to Health Care Act.
|
|
|
Current Status:
|
10/1/2025 - Referred to Committee Senate Health
|
|
|
State Bill Page:
|
https://www.legislature.ohio.gov/legislation/legislation-summary?id=GA136-SB-258
|
|
SB274
|
PROHIBIT MENTAL HEALTH SERVICES WITHOUT PARENTAL CONSENT (CIRINO J, BRENNER A) To prohibit the provision of mental health services to minors without parental consent.
|
|
|
Current Status:
|
10/1/2025 - Referred to Committee Senate Health
|
|
|
State Bill Page:
|
https://www.legislature.ohio.gov/legislation/legislation-summary?id=GA136-SB-274
|
|
SB295
|
RESTORATION OF COMPETENCY-CRIMINAL CASES (MANNING N, PATTON T) Relative to the timeline for restoration of competency in criminal cases and to declare an emergency.
|
|
|
Current Status:
|
2/20/2026 - SIGNED BY GOVERNOR; eff. 2/20/26
|
|
|
State Bill Page:
|
https://www.legislature.ohio.gov/legislation/legislation-summary?id=GA136-SB-295
|
|
SB299
|
REGARDING KRATOM PRODUCT SALES (BLESSING III L) Regarding sales of kratom products.
|
|
|
Current Status:
|
11/18/2025 - Senate General Government, (First Hearing)
|
|
|
State Bill Page:
|
https://www.legislature.ohio.gov/legislation/legislation-summary?id=GA136-SB-299
|
|
SB352
|
REGARDING BEHAVIORAL HEALTH SCREENINGS-PERINATAL PERIOD (WEINSTEIN C, TIMKEN J) Regarding behavioral health screenings in the perinatal period and to make an appropriation.
|
|
|
Current Status:
|
2/11/2026 - Referred to Committee Senate Finance
|
|
|
State Bill Page:
|
https://www.legislature.ohio.gov/legislation/legislation-summary?id=GA136-SB-352
|
|
|
Gov. DeWine’s Final State of the State Address – March 11th
Ohio Governor Mike DeWine will deliver his final “State of the State” address to a joint session of the General Assembly next month, per a resolution introduced and approved Wednesday in the House.
The chamber passed HCR36 (Manning), which sets Wednesday, March 11 as the date of the speech. The resolution still needs Senate approval which likely won’t happen until Wednesday, March 4 – the next day a Senate session is set at this point. It will begin at noon in the House Chambers. |
|
Affirming Families First Act Targets Local Control in Gender Identity
A proposed Ohio bill, House Bill 693 – the “Affirming Families First Act”, would significantly change state and local policies affecting LGBTQ+ youth, including overriding local protections and limiting how schools, agencies, and service providers address gender identity. Spanning 55 pages, the legislation touches parental rights, child welfare, education policy, and local government authority. Sponsors say the bill is intended to prevent government entities from promoting or affirming transgender and nonbinary identities.
A major provision would effectively reinstate conversion therapy in areas where it is currently banned by redefining the practice so that certain counseling aimed at discouraging transgender identity would not qualify as prohibited conversion therapy. Several Ohio jurisdictions — including Cleveland, Akron, Columbus, Cincinnati, and Cuyahoga County — currently maintain such bans. The bill would also restrict collection of sexual orientation and gender identity data by some public entities.
The legislation further addresses custody and child welfare, barring courts and agencies from penalizing parents who do not affirm a child’s gender identity and preventing foster or adoptive placement decisions based on caregivers’ views on transgender issues. In schools, it would limit requirements around use of students’ preferred pronouns and protect staff from discipline related to pronoun usage. The bill also establishes enforcement mechanisms, including potential state funding penalties for noncompliant local governments, and builds on prior laws restricting gender-affirming care and athletics participation for transgender minors.
The Ohio Council will continue to track this legislation as it works its way through the legislative process to assess potential impact on behavioral health practice and will keep Ohio Council members informed of any developments. |
|
Proposed HB 524 to Prevent AI that Encourages Self-Harm
At least four Ohio children have used artificial intelligence to write their suicide notes and lawmakers have introduced a bipartisan bill that would prevent anyone from creating an AI model in Ohio that encourages users to engage in self-harm or harm another person.
Ohio House Bill 524 would empower the Ohio Attorney General’s office to investigate and prosecute anyone who creates AI models that are responsible for creating technology that encourage self-harm, she said. According to a 2025 report from Common Sense Media, 72% of teenagers have used AI companions at least once, 52% interact with these platforms at least a few times a month, and 12% of teens use AI for emotional or mental health support. Lack of access to mental health resources could be driving people to turn to AI.
Out of Ohio’s 88 counties, 75 are mental health shortage areas, according to a recent study from the Health Policy Institute of Ohio. |
|
HB 718 Introduced – Establishing QMH & Certified Peer Support Credentials
After years of advocacy and collaboration with Ohio Council members and community partners, Ohio House Bill 718, “Revising the Chemical Dependency Professionals Board & Duties” has been introduced. This proposed legislation would transition Certified Peer Supporter credentialing to a professional licensing board as proposed by the administration during the last budget process and establish a 3-tiered Qualified Mental Health credential with clearly defined training, education, and scope of practice. The Ohio Chemical Dependency Professionals Board name would be changed to the “Behavioral Health Professionals Board” (BHPB), and would require BHPB to certify both, Certified Peer Supporters (CPS) and Qualified Mental Health (QMH) Professionals, while making other changes to the laws governing the Board and the professional classifications it currently regulates.
The proposed QMH and CPS certifications seek to improve patient protections by codifying scopes of practice and ethical guidelines for practice and bring an added sense of professionalism for more than 21,000 paraprofessionals already delivering behavioral-health related services across Ohio. The provisions would streamline processes for certification and establish professional competencies to deliver care, while also addressing current behavioral health workforce shortages by creating new degree and non-degree pathways into a career in behavioral health. The credential is portable across employment sites and reduces training and retraining experiences each time the individual changes employers, which will result in reduced training and onboarding costs for community behavioral health providers, as newly hired QMH credentialed individuals will have a base level of experience, training, and education consistent with the requirements of the credential that is travels with them across employment sites.
Notably, HB 718 will directly respond to Ohio’s current Mental Health Professional shortage, by creating new opportunities to attract and recruit individuals into the mental health job sector. The QMH tiered credentialling structure creates a pathway for growth and development that is important in job retention. It opens new opportunities to create career tech programs, apprenticeships, and career development initiatives specifically in the mental health sector that have been limited due to the lack of a viable credential below the master’s degree level; and aligns with 8-out of-22 goals in the Department of Behavioral Health’s (formerly the Ohio Department of Mental Health & Addiction Services) Behavioral Health Workforce Roadmap, which outlined 22 initiatives to implement by 2027 to address Ohio’s current BH workforce needs; and is directly responsive to Prioritized Initiative #11, “Add licensure capabilities for those with a 4-year psychology or sociology degree” and Prioritized Initiative #15, “Develop certifications that can be achieved by starting into the behavioral health field at the career center level in high school”.
The Ohio Council will be actively supporting this legislation as it moves through the committee and public hearing processes and will keep members informed of any developments or opportunities to provide testimony. We would like to sincerely thank all our members who contributed thoughts and feedback regarding this proposed legislation over many years of engagement. We would not have reached this new milestone without your partnership, expertise, and commitment to strengthening our profession and improving lives. |
|
OhioPRO Begins Statewide Peer Recovery Supporter Trainings
The Ohio Department of Behavioral Health is pleased to announce that we have partnered with Ohio Peer Recovery Organizations (OhioPRO) to offer statewide Peer Recovery Supporter (PRS) training. Online PRS trainings, including day, evening, and weekend options, will be scheduled at a regular cadence and will be open to all prospective Certified Peer Recovery Supporters (CPRS) in Ohio.
Local ADAMHS boards and board-designated host organizations will continue to host in-person training that prioritize prospective CPRS within the board area, with OhioPRO managing registration.
In collaboration with DBH, OhioPRO will serve as the centralized contact for all PRS Trainings statewide, providing streamlined registration and shorter waits to register for PRS training. Future PRS trainings will be announced on the DBH website and in the BH Bulletin. |
|
New CDCA-Pre & CDCA Training Requirements Effective July 1st
As a reminder, new changes to CDCA-Pre and CDCA Requirements go into effect July 1st. The implementation date was pushed back from March 1st to support organizations in meeting the new requirements. These changes are intended to strengthen the foundation and ensure consistency of substance use disorder counseling education, and impact what education/trainings will be accepted to apply for initial CDCA Preliminary and CDCA certifications.
Effective July 1, 2026 – the Ohio Chemical Dependency Professionals Board (CDP) Board will no longer be accepting single CEU’s or CEU packages for initial applications and will only be accepting college courses OR a CDP Board approved continuing education CDCA Bundle.
These changes will also improve efficiency of CDCA application reviews.
For further information, please click here CDCA Certification Changes
Any questions about these changes or Educational Providers interested in submitting a Bundle, please contact Esha Thakar @ [email protected]. |
|
DCY Announces Child Wellness Campuses
Governor Mike DeWine and the Ohio Department of Children and Youth (DCY) have announced funding support for six child wellness campuses across Ohio. The campuses will provide short-term, therapeutic care for children and youth with complex needs, helping keep them closer to their families, schools, and communities.
In partnership with the Ohio General Assembly, Governor DeWine directed $20 million from Ohio’s operating budget to support the creation of four new child wellness campuses and the expansion of two existing campuses. Together, the funded campuses will expand Ohio’s capacity to serve children and youth with complex needs in settings designed specifically for stabilization and healing.
The following communities/organizations were selected to receive funding:
- Talbert House Inc., Hamilton County
- Unison Behavioral Health Group, Northwest Ohio
- Safe Opportunity Foster Alliance, Southeast Ohio (Expansion)
- Buckeye Ranch Inc., Central Ohio
- Cleveland Christian Home Inc., Cuyahoga County (Expansion)
- Champions Bridge, Franklin County
|
|
DBH Announces Adult Mobile Crisis Pilot
The Ohio Department of Behavioral Health (DBH) announced the selection of two applications for the Adult Mobile Crisis (AMC) pilot project. The selected applicants are the Hamilton County Mental Health and Recovery Services Board (MHRSB), serving the Summit region, and the Mental Health and Recovery Services Board (MHRSB) of Lucas County, serving the Northwest region.
The Hamilton County MHRSB will pilot a co-responder staffing model, while the MHRSB of Lucas County will pilot a clinician-led staffing model. The AMC pilot project will begin with an eight-week readiness phase designed to support awardees and their local partners in achieving a successful project launch.
DBH has contracted with Advocates for Human Potential, (AHP) Inc., to conduct an independent evaluation of the two staffing models during the pilot period. AHP will collect, review, catalog, and analyze data and outcomes to assess whether one or both models demonstrate preliminary effectiveness and to establish a data foundation to inform future strategic direction with AMC services in Ohio. |
|
OhioRISE Eligibility Proposed Rule – OAC 5160-59-02
The Ohio Department of Medicaid (ODM) has proposed revisions to the OhioRISE eligibility rule that would align enrollment timing with managed care by establishing a first-of-month effective date when eligibility criteria are met. The change is intended to improve consistency across Medicaid managed care enrollment processes.
The Ohio Council recently submitted comments on the proposal, focusing on implementation considerations. In our comments, we noted that the first-of-month effective date and retroactive termination provisions may have implications for billing, payment responsibility, and cross-payer coordination when services are delivered earlier in the same month.
We encouraged ODM to provide further guidance to support consistent implementation across plans and providers. The Ohio Council will continue to monitor updates as the rule moves forward. |
|
OBM Issues Memo on Proposed Property Tax Elimination Impact
The Ohio Office of Budget & Management (OBM) has issued a memo outlining the potential impact of a proposed statewide ballot initiative that would eliminate all property taxes throughout the state of Ohio; which would negatively impact a critical source of revenue that currently supports schools, police, fire departments, emergency services, and other critical services statewide. memo provides a high-level summary of the impacts of such an amendment; if the issue makes the ballot, OBM will provide a detailed analysis in accordance with Ohio Revised Code Section 3519.04.
While the State of Ohio does not collect property taxes, Ohio’s cities, counties, counties, townships, and school districts have long depended on them to pay for the services residents rely on every day. Today, property taxes, including real property and public utility personal property taxes, generate about $24 billion each year for local governments across the state. To put this into perspective, that’s equal to the total revenue from Ohio’s state income and sales taxes combined.
Replacing this budget deficit would require either an increase in state income tax or sales tax. According to analysis by the Tax Foundation, income tax rates across Ohio would need to quadruple or more, reaching 11–15 percent statewide, to replace local property tax levies. OBM, after consulting with the Ohio Department of Taxation, estimates that replacing local property tax would require state sales tax rates approaching 15–18 percent, significantly higher than any other state.
The Ohio Council will closely monitor information regarding this proposed ballot initiative and will keep Ohio Council members informed of any changes or developments. |
|
Ohio Capital Budget Requests Due By March 12th
The Ohio General Assembly is currently working to compile capital budget requests. Ohio House and Senate members must submit project requests to leadership by 12:00pm on March 12th. Organizations who are interested in pursuing funding for capital projects or expenses should contact their local officials as soon as possible to discuss their requests. OMB shared a helpful guidance document and offering tips on how to secure funding for “community projects” within the Capital Budget. As always, members who need assistance identifying or connecting with their local legislators are welcome to reach out to the Ohio Council for support. |
|
NHSC Loan Repayment Applications Open Through March 31st
The National Health Service Corps (NHSC) Loan Repayment Application with the Health Resources Services Administration (HRSA) is now open through March 31st at 7:30pm. Clinicians who provide direct clinical care under the following disciplines and specialties can apply:
- Primary Care
- Oral Health Care
- Behavioral Health Care
Full-time service repayment may qualify an applicant to receive up to $75,000 for a two-year service obligation for primary care providers assigned to a primary care HPSA; and up to $50,000 for a two-year service obligation for behavioral health and oral health care providers assigned to a mental health or dental HPSA.
NHSC clinicians must work at an NHSC-approved site located in a HPSA, which can be found around the country in rural, urban, and frontier communities. NHSC-approved sites are generally outpatient facilities providing primary care, oral, and/or behavioral health services. Visit the Health Workforce Connector to search for training and employment opportunities at NHSC-approved sites.
For more information:
|
|
ACA Enrollment Declines Following Tax Credit Expiration
Data released by the Centers for Medicare and Medicaid Services shows that 469,616 Ohioans enrolled in Affordable Care Act (ACA) marketplace coverage in the open enrollment period that ended Jan. 15, a decrease of nearly 114,000 from last year. This decline comes following the expiration of enhanced premium tax credits at the end of 2025, which caused out of pocket costs for Marketplace insurance to skyrocket.
A brief compiled by the Health Policy Institute of Ohio (HPIO) highlights these federal figures, which indicate that Ohio experienced roughly a 20% drop in ACA exchange enrollment for the 2026 plan year, ranking it among the states with the largest declines in the nation, exceeded only by a few states including North Carolina, Georgia, and Florida. The total drop in enrollment nationwide was 5%; making Ohio’s reduction four-times larger than the national average.
These trends are important for providers to consider as you evaluate payer mix, budget planning, and uncompensated care needs. A shrinking insured population typically translates into a higher proportion of uninsured patients and greater financial pressure on safety-net providers. Providers and ADAMH boards may want to factor these enrollment shifts into their forecasting and resource allocation strategies for 2026 and beyond. |
|
Executive Order Creating the Great American Healthcare Initiative
The Trump Administration issued a new Executive Order (EO) directing the U.S. Department of Health & Human Services (HHS) to coordinate a federal government response to the substance use and addiction crisis, along with a corresponding fact sheet.
The “Great American Recovery Initiative” will be chaired by HHS Secretary Robert F Kennedy Jr. and Senior Advisor for Addiction & Recovery, Kathryn Burgum, and will advise federal agencies on how to integrate programs on drug prevention, early intervention, treatment, recovery support, and reentry.
The initiative is also tasked with consulting states, tribal nations, local governments, community and faith-based organizations, the private sector, and philanthropic partners to identify effective recovery strategies to ensure more Americans receive lifesaving care and support.
The EO directs Secretary Kennedy to launch an initiative to coordinate a comprehensive federal response to the addiction crisis by aligning programs across agencies, setting clear goals, and providing data-driven public updates on progress. It emphasizes increasing awareness of addiction as a disease, expanding access to treatment, and fostering a culture that supports and celebrates recovery. The Initiative will also advise federal agencies on integrating prevention, early intervention, treatment, recovery supports, and re-entry services, guide the strategic use of grants to strengthen prevention, treatment, and long-term resilience, and consult with states, tribal nations, local governments, community- and faith-based organizations, the private sector, and philanthropy to ensure more Americans receive needed care and support recovery efforts.
In alignment with this EO, RFK also announced a $100M investment in the Great American Recovery Initiative through the STREETS program, aligned with the Ending Crime and Disorder on America’s Streets executive order. The announcement reports this investment is the centerpiece of the Great American Recovery and is designed to solve long-standing homelessness issues, fight opioid addiction, and improve public safety by expanding treatment that emphasizes recovery and self-sufficiency. The STREETS initiative will fund targeted outreach, psychiatric care, medical stabilization and crisis intervention, while connecting Americans experiencing homelessness and addiction to stable housing with a clear focus on long-term recovery and independence. In addition, $10 million was announced for Assisted Outpatient Treatment (AOT). |
|
USDOE Proposes Changes to Graduate Degrees
Pursuant to provisions of H.R.1, the U.S. Department of Education (DOE) recently issued a Notice of Proposed Rulemaking limiting graduate federal students loans. The proposed changes that may result in several graduate degrees, including nursing, social work and some counseling degrees, no longer being classified as “professional” programs. This change would limit the maximum available loan amounts for graduate students pursuing advanced degrees in these fields.
The proposal would limit the annual amount of public loans an individual can obtain for graduate degrees to $20,500 per year and $100,000 over the course of one's lifetime. Medicine, osteopathic medicine, podiatry, chiropractic, optometry, pharmacy, dentistry, veterinary medicine, law, theology and clinical psychology would still be considered professional degrees, for which students can receive up to $50k per year and $200k total in public loans. Previously, graduate students could borrow up to the cost of attendance.
The DOE asserts on their “Myth vs. Fact” webpage that limiting the amount of loans available to degree programs with “modest earning potential” will drive down the prices of these degree pathways, citing that universities have irresponsibly raised tuition prices; and asserts that those who are concerned that this will have a negative impact on workforce challenges are engaging in “fear mongering” tactics. They claim that, while it is not yet in effect, the Act’s federal loan caps are already reigning in inflated prices of graduate programs across the country.
Nevertheless, the Ohio Council submitted comments urging the DOE to reconsider the classification of behavioral health (BH) graduate programs, and to continue recognizing them as professional degree programs and essential health and human services pathways; citing that such changes would make it harder to obtain a degree in BH-related fields, further exacerbating the mental health workforce crisis. You have the opportunity to comment on this proposed rule by Monday, March 2. You are welcome to use our comments as a template. When you're ready to submit your comment, follow the green “Submit a Public Comment” button on the proposed rule’s Federal Register page and follow the instructions.
Related resources providing additional background information include a summary of the proposal from Inside Higher Ed, a press release from DOE, and some information from NASW FL. If the rule is finalized, it would be effective July 1, 2026. |
|
CMS Updates Core Quality Measure Sets on Health Outcomes
The Centers for Medicare and Medicaid Services (CMS), through the Core Quality Measures Collaborative (CQMC) announced updates to nine of its core measure sets for 2025, sharpening the focus on outcomes, addressing key gaps in existing sets, and removing measures that are outdated, redundant, not in use, or no longer necessary as performance is universally high.
The CQMC is a public–private partnership convened by AHIP and the Centers for Medicare & Medicaid Services (CMS). It includes more than 75 organizations representing patients, purchasers, health plans, providers, and quality experts that work together to promote aligned, high-value core quality measures for use in value-based care.
For the 2025 update, the CQMC concentrated on three priorities:
- Addressing key gap areas where the existing measures did not fully capture high-priority aspects of care, including patient experience, care coordination, and specialty-specific performance.
- Adding new outcome-focused measures that reflect performance on complications, disease control, and avoidable utilization.
- Removing measures that are outdated or not in use to keep the core sets relevant, feasible, and parsimonious for value-based payment arrangements.
The CQMC core sets cover major clinical domains commonly used in alternative payment models and other value-based arrangements, and are designed to streamline measurement so health plans and clinicians can rely on a concise list of measures that support performance improvement and comparability across programs.
The 9 CQMC domains include:
|
|
CMS Site Visits
The Centers for Medicare and Medicaid Services (CMS) shared a reminder that they have the authority to conduct site visits to verify the operational status of any enrolled sites. Site visit inspectors carry a photo ID and CMS-issued letter of authorization that you may review but not retain or copy. Starting January 3, 2026, two new site verification service contractors will conduct these visits:
- East: Arch Systems, LLC
- West: Signature Consulting Group
|
|
Medicare Telehealth Waivers – Extended through Dec 31, 2027
President Trump signed the Consolidated Appropriations Act, 2026 (CAA, 2026), which includes extending Medicare telehealth flexibilities through December 31, 2027. This includes an extension of the waiver of the requirement for practitioners who provide behavioral and mental health services via telehealth to furnish in-person visits within six months of the first telehealth visit and annually thereafter.
Separately, CMS updated the MLN outlining Medicare’s telehealth requirements. However, it defers to CMS and HHS resources on specific details and does not explicitly outline the extension of the flexibilities mentioned above. |
|
42 CFR Part 2 Changes Now In Effect – Resources on Enforcement
Changes to 42 C.F.R. Part 2 went into effect February 16th, 2026. These changes modify the Confidentiality of Substance Use Disorder (SUD) Patient Records regulations to create better alignment with HIPAA. Our partners at Vorys, Sater, Seymour and Pease have shared the following information regarding anticipated launch of the HHS Civil Enforcement Program for Part 2 implementation:
In conjunction with the effective date of various updates to 42 CFR Part 2, the U.S. Department of Health and Human Services (HHS) Office for Civil Rights (OCR) launched its new enforcement program pertaining to the confidentiality of substance use disorder (SUD) records. Specifically, OCR is implementing various civil enforcement mechanisms as required under the Coronavirus Aid, Relief, and Economic Security (CARES) Act and its implementing regulations under 42 CFR Part 2.
Per its announcement on February 13, 2026, OCR’s enforcement program will:
- Investigate compliance with 42 CFR Part 2 including required updates to Notice of Privacy Practices (NPPs) (see Model Notice templates here) and the new breach notification requirements;
- Accept complaints of alleged Part 2 confidentiality violations;
- Accept breach notification, as specified under the Health Insurance Portability and Accountability Act (HIPAA), for breaches of confidentiality of SUD records; and
- Resolve noncompliance findings through various civil enforcement mechanisms including resolution agreements, monetary settlements, corrective actions, or civil monetary penalties.
Given that the changes to 42 CFR Part 2 were intended to align Part 2 with HIPAA, it is anticipated that we may begin to see Part 2 enforcement trends track the HIPAA enforcement activity immediately after the introduction of the Health Information Technology for Economic and Clinical Health Act (HITECH). For example, several early enforcement cases involved failure to safeguard ePHI, resulting in settlements ranging from $150,000 to $1.7 million. In another case, a provider agreed to a settlement of $275,000 for the disclosure of PHI without patient consent.
Now that OCR has a new enforcement mechanism in place, to date, OCR has settled around 150 enforcement actions, totaling approximately $150 million in penalties. For questions regarding these changes, please seek guidance from your organization’s legal counsel. The Ohio Council will continue monitoring implementation of the new 42 CFR Part 2 implementation and will keep Ohio Council members informed of any additional pertinent information. |
|
Congressional Update
At the beginning of February, President Trump signed legislation to partially end a government shutdown, moving forward $1.2T in appropriations. While the bill was not inclusive of Department of Homeland Security funding or a solution for the recently expired ACA Enhanced Premium Tax Credits, it did include appropriations for the Department of Health and Human Services (HHS) that would impact behavioral health. If another partial shutdown does occur, HHS programs would not be impacted.
Total funding for the Substance Abuse and Mental Health Services Administration (SAMHSA) was provided at $7.4 billion, relatively level to FY24 funding, when appropriations bills were last previously enacted. (FY25 saw a yearlong continuing resolution rather than an appropriations bill.)
Overall, many mental health and substance use programs saw level or slightly increased funding. This is a tremendous win for the field, particularly in a challenging fiscal environment.
The Labor, Health and Human Services, Education, and Related Agencies (LHHS) agreement also extends Medicare telehealth flexibilities through the end of 2027, including a delay of in-person requirements for Medicare telehealth services for mental health under Medicare.
Additional language in the agreement includes a requirement that HHS notify the committee at least three days prior to announcing or providing notice of a grant termination. It also directs SAMHSA to consult with Congress before issuing a funding opportunity announcement. This language provides additional congressional oversight in the agency grantmaking process.
For additional information:
The Ohio Council will continue to monitor developments related to the federal budget and will keep Ohio Council members informed of any changes or potential impacts. |
|
Engage, Empower, Treat: A Behavioral Health ECHO Learning Series
AmeriHealth Caritas Ohio, in collaboration with Project ECHO, is excited to launch Engage, Empower, Treat: A Behavioral Health ECHO series — an emerging case-based learning model for practitioners. Continuing education for providers who participate in this series will be applied for through Arizona State University, for physicians and nurses, and the Ohio Counselor, Social Worker, and Marriage and Family Therapist (CSWMFT) Board for social workers, licensed professional counselors, and marriage and family therapists. This opportunity doesn’t cost anything for participating AmeriHealth Caritas Ohio practitioners. Please read on for more information and register to join this ECHO model clinic.
The Extension for Community Healthcare Outcomes (ECHO) model was developed by the University of New Mexico Health Sciences Center and is now used nationwide and internationally. To sign up for the virtual ECHO series, please email [email protected]. Further registration instructions will be emailed to you.
| Date |
Topic |
March 12
12:00 PM - 1:00 PM |
Reframing Addiction: A Chronic Disease Approach to Treatment and Recovery |
April 9
12:00 PM - 1:00 PM |
Zero Suicide Using the Trauma-Informed Care Model |
May 14
12:00 PM - 1:00 PM |
Managing Behavioral Health Conditions During the Perinatal Period |
June 11
12:00 PM - 1:00 PM |
Attention Deficit Hyperactivity Disorder (ADHD) in Adults |
July 9
12:00 PM - 1:00 PM |
Start the Conversation: Assessment and Intervention for Alcohol Use |
What is the ECHO model?
The ECHO model facilitates case-based learning for front-line practitioners via teleconferencing clinics. Similar to virtual chart
rounds, the ECHO model creates a space where practitioners can share knowledge and build support to better manage patients with complex care needs.
For more information on Project ECHO, please visit https://echo.unm.edu.
What’s the goal of this program?
Engage, Empower, Treat: A Behavioral Health ECHO Learning Series exists to:
- Provide education to increase screening and treatment of behavioral health disorders among members in physical health settings.
- Recognize symptoms, adaptations, or somatic complaints in response to a traumatic experience.
- Build skills to successfully engage members in treatment through motivational interviewing and harm reduction interventions.
Click here to view the event flyer! |
|
16-Hour Certified Peer Recovery Support Training Curriculum Available in Ohio Learn
The 16-hour Certified Peer Recovery Supporter Training Curriculum is now available in Ohio Learn! In Ohio, to apply for certification as an Adult Peer Recovery Supporter, apply for certification as a Youth Peer Supporter, or to be eligible to supervise peer supporters, individuals must complete the Ohio Learn 16-hour Certified Peer Recovery Supporter Training Curriculum. This free training series must be completed before registering for the DBH 40-hour Adult Peer Recovery Supporter Training or the DBH 40-hour Youth Peer Supporter Training. Please visit this webpage for instructions to complete the curriculum.
Click here to find a walkthrough of the Ohio Learn registration process, including pictures of each step.
IMPORTANT REMINDER REGARDNG EBASED ACADEMY: If you previously completed the certified Peer Recovery Supporter training learning plan on eBased Academy, please note that the eBased Academy website is retiring February 28, 2026.
What do you need to do before this date?
- If you have started the Certified Peer Recovery Supporter Training Learning Plan in eBased Academy, you must complete all modules and save your completion certificate to your computer by February 28, 2026. If you are partway through the learning plan on February 28, your progress will NOT transfer to Ohio Learn (you will need to start the learning plan over).
- If you have completed the Certified Peer Recovery Supporter Training Learning Plan in eBased Academy, you must download and save to your computer your certificate of completion. You will no longer have access to the certificate after May 31,2026. DBH will not be able to provide you with a copy of your certificate once the eBased Academy website is retired. To obtain a copy of your completion certificate after May 31, 2026, you will need to re-take the learning plan in Ohio Learn.
- If you have not yet started the 16-hour Certified Peer Recovery Supporter Training Curriculum, please visit this webpage for instructions to begin the curriculum in Ohio Learn: https://dbh.ohio.gov/community-partners/peer-supporters/resources/ohio-learn/ohio-learn
|
|
January 2026 Edition
Federal Policy & Legislation
State Policy & Legislation
Reports & Resources
Training & Events
|
|
2026 OHSAA Youth Gambling Survey Now Open
Ohio for Responsible Gambling (ORG), in partnership with the Ohio High School Athletic Association (OHSAA), invites students in grades 9–12 to take part in the 2026 Youth Gambling Survey. The short, anonymous survey helps identify youth attitudes and behaviors related to gaming and gambling. Results will guide prevention and education efforts led by ORG’s Change the Game Ohio campaign.
Spread the Word: Help ORG reach more students by sharing this announcement in your newsletters, team updates, or community networks. Together, we can build a safer, more informed future for Ohio’s youth.
Take the survey at Youth Gambling Survey 2026. The deadline to complete the survey is March 16.
If you have questions or would like additional information, please contact Susan Diamond at [email protected]. |
|
Participate Today in Developing a PEER Supervisor Training Curriculum
Across Ohio, peer support teams are growing and expanding into new settings, making Peer supervisors more necessary than ever. As such, OhioPRO has announced the launch of an initiative to develop a new Peer Supervisor Training Curriculum.
To support this work, OhioPRO will engage with peer supporters, peer supervisors, and recovery leaders to co-create a curriculum that promotes excellence and is rooted in OhioPRO’s values. OhioPRO invites stakeholders to participate in the development of this standardized curriculum.
There will be multiple opportunities to contribute, including focus groups, listening sessions, interviews, and surveys. If you are interested in participating your perspective to help shape this curriculum, please complete this interest form. |
|
New Research: Science Suggests Different Psychiatric Dx Might Have the Same Cause
A sweeping new study of psychiatric and genetic records has the potential to change treatment for millions of psychiatric patients, finding that many conditions involve similar genes and may not need to be treated as distinct illnesses.
Half of all people will experience a psychiatric disorder in their lifetime, and more than half of those patients will be diagnosed with a second or third disorder. If the research findings are accurate and there is a common genetic predisposition for multiple differing types of psychiatric conditions, then this could open opportunities for screening, early identification, and new treatment methodologies.
Published in Nature, the paper addresses the boundaries psychiatry uses to separate similar conditions like bipolar disorder and schizophrenia. In essence, the study suggests that bolstering the traditional emphasis on patient behavior with a deeper understanding of the biology of mental illness could lead to better treatment. The research also suggests that linking genes to the brain processes they influence will provide psychiatrists with greater insight into their patients, and guide researchers toward new risk factor identification, genetic testing opportunities, or other therapies. |
|
New Study: Psychological Therapy & Psychedelic-Assisted Therapy in Treating Depression
Psychedelic-Assisted Therapy (PAT) is a novel intervention for depressive symptoms, typically delivered with additional psychological therapy sessions. A new systemic review of 12 controlled clinical trials with 733 participants sought to evaluate how psychological therapy pre-and-post PAT treatment impacted clinical outcomes.
Although a combination of pharmacological and psychological therapy is almost universally employed in PAT protocols, most research to date has been primarily focused on the safety and efficacy of the psychedelic substance itself, leaving the psychological therapy components poorly understood and without clear guidelines. This lack of systemic research has led to uncertainty about whether or not psychological therapy in general is even necessary; or if psychedelic experience alone is sufficient to drive therapeutically meaningful change.
The results, published in JAMA, found that a greater quantity of preparation therapy (prior to administering PAT) resulted in significantly larger reductions of depressive symptoms. These findings highlight a potential key role of preparation in optimizing PAT outcomes, contributing to a growing volume of evidence that traditional counseling services and interventions can work cooperatively with new pharmacological interventions with PAT.
Likewise, longer follow-up durations after PAT were linked to smaller symptom reductions, sustaining the treatment outcomes for a longer duration. Researchers suggest that this is a potential area for future research or trials, that could aim to standardize follow-up intervals and examine symptom trajectories over longer time frames to better understand maintenance and relapse patterns.
Overall, the implications of these results provide evidence that the efficacy of psychedelic treatment models is likely shaped substantially by the therapeutic context in which it is embedded. For more information, read the full journal article here. |
|
New Research: Psychologists Express Worry over A.I. Tools
As more psychologists adopt AI tools, there is also growing awareness about artificial intelligence tools, especially with respect to patient safety and data privacy.
A majority of psychologists said they are concerned about potential harms of this technology, with more than 60% saying they are worried about potential data breaches, biased inputs and outputs and social harms. Many also expressed concerns about hallucinations, where the platforms fabricate facts or present inaccurate information.
Even with the concerns, however, nearly 56% of psychologists recently surveyed by the American Psychological Association responded that they are using some AI tools in their practices. That's significantly higher than the 29% who said the same last year. And nearly a third of respondents said they use these tools on a monthly-basis; up by more than two-fold since last year.
Psychologists are seeing potential opportunities to incorporate AI into their practices, by making their work more efficient, which could have downstream effects to reducing burnout, reducing those aspects of the workplace that people don't particularly enjoy. |
|
New Study: Association Between Adult-AI Use and Depressive Symptoms
The use of generative artificial intelligence (AI) has increased massively since the introduction of ChatGPT 3.5 (OpenAI) in late 2022. Along with enthusiasm for the potential benefits of these tools, anecdotal evidence of potential harms to mental health has emerged, with suggestions that use of chatbots may precipitate or exacerbate delusions in vulnerable individuals and even contribute to risk for suicide attempts in rare cases.
In a recent study funded in part by the National Science Foundation, researchers analyzed data drawn from the Civic Health & Institutions Project (CHIP-50) study, which surveyed 20,847 individuals 18 and older across all 50 states. Key markers that were explored included frequency of AI use and social media use. They compared these responses to data collected from those same individuals through a PHQ-9 questionnaire.
Researchers found that daily AI use was common and significantly associated with depressive and other negative affective symptoms, after adjusting for sociodemographic features. Notably, among individuals aged 45 to 64, the odds of reporting at least moderate depression were 50% greater for daily AI users.
Given the rapidity of AI dissemination and the scale of use, these results in aggregate suggest an immediate need to better understand potential causation and heterogeneity of outcomes. The picture that is emerging, however, is consistent with previous observations regarding social media use. Most social media literature, as with this study, is cross-sectional and correlative. Prolonged social media use has been related to mental health decline. Researchers also suggest that the differential associations in age strata warrant additional exploration to understand underlying factors across these subgroup associations, and whether or not some individuals may be more apt to experience depressive symptoms based on age or other factors.
For additional information, read the full study published in JAMA here. |
|
Open A.I. Makes Healthcare Push
Open AI, the parent company of ChatGPT, has set its sights on healthcare, and is part of a growing number of AI companies looking to make inroads in healthcare. The company has made a series of announcements in recent weeks that emphasize its interest in putting ChatGPT into the hands of patients and providers. Open AI’s move into healthcare includes two primary programs: “ChatGPT Health” and “Open AI for Healthcare”.
What is ChatGPT Health?
ChatGPT Health will allow patients to upload their medical records, including lab results, visit summaries, and clinical history, into the ChatGPT interface. The large language model will use information to help patients understand test results, prepare for doctor’s visits and understand what diets can help with their health.
Additionally, the company said it is working with several health tech companies on the product. Function Health, which closed a near-$300 million funding round in November and Weight Watchers will connect their applications to ChatGPT Health. Through those connections, ChatGPT can recommend lab insights from Function and dieting tips from Weight Watchers. The company also said users of Apple Health will be able to share their wellness and health data with ChatGPT to analyze the information.
What is OpenAI for Healthcare?
OpenAI’s enterprise product, which is available, gives health systems the ability to embed GPT-5 large language models into their workflows. It also gives them access to templates to help them create generative AI models for common use cases. Providers also can create clinical AI models that are drawn from peer-reviewed research studies, public health guidance and clinical guidelines. The tools are designed to help health systems implement clinical, operational, and research-driven large language models.
Consumer and Industry Response
The company has said that daily, 40 million people use ChatGPT for healthcare related purposes. They assert that because getting health advice is already one of the most popular uses for ChatGPT, the move to prioritize improvement of healthcare analysis and support was a natural next step during the development of GTP-5’s most recent update; and claim that there is a waiting list for consumers to use the ChatGPT Health functionality.
Additionally, OpenAI said it worked with several health systems on their enterprise product, OpenAI for Healthcare, including HCA Healthcare, Boston Children’s Hospital, Stanford Medicine Children’s Health, Memorial Sloan Kettering Hospital, Advent Health, and others. Boston Children’s Hospital, in particular, has had a multi-year partnership with OpenAI, where they developed a generative AI prompt library that helps the hospital’s employees with a wide range of tasks.
Source: “Open AI’s Massive Healthcare Push: Here’s What to Know”, by Modern Healthcare |
|
New Resource: Bullying & Suicide Prevention
Bullying can have serious and lasting effects on mental health, relationships, and a person’s sense of safety. People of all ages can be targets, and these experiences can contribute to anxiety, depression, and suicidal thoughts.
The Ohio Suicide Prevention Foundation (OSPF) recently released a new one‑pager that highlights warning signs, protective factors, and resources to help individuals, families, and communities prevent bullying and support those affected.
View the Bullying & Suicide Prevention Resource here, or click here for more OSPF suicide prevention resources. |
|
New Resource: SUD Treatment Month
The Ohio Department of Behavioral Health (DBH) is recognizing January as National Substance Use Disorder #Treatment Month. This year's theme is "Treatment Works! Find the Path that Works for You." Help raise awareness and share resources that connect people to treatment by downloading and sharing content available at samhsa.gov/treatment.
Also, Dry January is a great time to reset and recharge. If you know someone looking to take a break or make a change from alcohol or other substances, you can support them in seeking help. Find helpful resources to get the conversation started at samhsa.gov/families. For more ideas to help you explore your relationship with alcohol and tips for cutting back, visit the National Institute on Alcohol Abuse and Alcoholism's (NIAAA) Rethinking Drinking website, and be sure to check out the self-screening tool and alcohol misuse campaign resources available on the DBH website. |
|
Deadline Extended: National Survey of Mobile Crisis Programs
The New York State Psychiatric Institute (NYSPI) has announced the launch of a National Survey of Mobile Crisis programs, and the deadline has been extended through the month of February, now closing February 28st. Ohio is one of 5 partner states for this project, and they are aiming for 100% response rate from Ohio’s programs to expand their understanding of the various types of mobile crisis programs operating throughout the state. To date, only 21 programs have responded from Ohio.
With strong participation from Ohio, the state will be eligible to receive a dedicated report highlighting Ohio’s crisis services and statewide insights. Individual participants will be entered to win a $50 gift card. The survey takes approximately one-hour to complete.
The survey is hoping to collect data related to service types/areas; partnerships; program/team structure, training, technology, financing, and data collection.
Who should respond? The survey is seeking to target a wide range of programs, including behavioral health provider-mobile crisis programs, mobile response and stabilization services (MRSS), law enforcement-based co-responder programs, and alternative or community responder programs. Specifically, individuals in leadership positions (Executive Director/CEO, Program Directors/Managers, Clinical Supervisors, or other supervisory staff) would be best suited to submit responses on behalf of their organization.
Questions can be directed to Matei Vohr, Project Manager, at [email protected]. |
|
DBH Report: 2026 OH Problem Gambling Services Report
The Ohio Department of Behavioral Health (DBH) recently released the SFY 2025-26 Ohio Problem Gambling Services Annual Report and Plan.
The report, compiled by DBH’s Office of Community and Family Resiliency, offers an in-depth look at the continuum of care from prevention to recovery designed to support communities, individuals, and families affected by gambling-related harm. Beyond clinical services, the report underscores the vital role of public awareness, workforce development, and integrated service delivery in building a responsive, person-centered system of care. It also highlights those collaborative efforts of Ohio for Responsible Gambling partners (ORG), including the Ohio Casino Control Commission (OCCC), the Ohio Lottery Commission, and the Ohio State Racing Commission, whose shared commitment strengthens the reach and impact of these initiatives.
Read the full 2025-2026 report here.
|
|
HPIO Report: Access to MH Care for Ohio Children & Youth
The Health Policy Institute of Ohio (HPIO) has released a new report, “Access to Mental Health Care for Ohio Children & Youth”, highlighting the challenges that continue to persist across the state of Ohio for youth and families seeking to access behavioral health supports.
Many Ohio children and youth are struggling with mental health conditions. Early identification and treatment can keep them on a path toward well-being; however, according to a new analysis from HPIO, families continue to encounter various types of barriers to accessing care. These barriers include workforce challenges and provider shortages, the increasingly high cost of care, and difficulty navigating our complex health and insurance systems.
An interesting finding of the report emphasizes increasing difficulties accessing care, particularly for families with private (i.e., commercial) health insurance. 45% of parents/caregivers with private insurance found it somewhat or very difficult to access care, compared to only 30% with public insurance, highlighting a continued need to try and bring consistency to reimbursement rates across all payor types.
Additional findings included affirmation that MH workforce shortages continue to persist at all levels, especially among clinicians who are trained to care for children with the most intensive needs. In 2025, 75 of Ohio’s 88 counties (or 85.2% of the state) was designated, according to the Health Resources Services Administration (HRSA), as a Mental Health Professional Shortage Area (MHPSA). While this number remains unchanged from 2024 MHPSA data, it is a stark increase from just 2021, where only 76% of the state held this designation. Finally, inconsistent data on MH care access in Ohio, which would allow policymakers to better understand gaps in access and more strategically direct attention ad resources to fill those gaps.
For additional information:
|
|
HRSA Report: National Survey of Children’s Health Data Released
This January, the Health Resources Services Administration (HRSA) has released results of the 2024 National Survey of Children’s Health (NSCH). The NSCH is the largest, most comprehensive national- and state-level dataset on the health and well‐being of America’s children, their families and their communities.
The Healthy Behaviors among School-aged Children Data Brief presents findings on healthy behaviors among school-aged children (6-17 years) and their relationship to chronic conditions and obesity. Healthy behaviors include limiting intake of sugary drinks, getting adequate sleep, limiting screen time and getting at least one hour of physical activity every day.
The NSCH provides data on a range of other indicators, such as the prevalence and impact of special health care needs, health care quality and access, physical and mental health, and adverse childhood experiences. We encourage our partners to use the new 2024 data to better understand the strengths, needs, and health service gaps of America’s children, and to support progress toward solutions that promote their optimal health and well-being.
Watch HRSA’s NSCH 90-second video and share it so more people learn about and use this valuable resource. |
|
HRSA Releases Health Workforce Dashboard Update
The Health Resources Services Administration (HRSA) has released updated health workforce dashboards and data resources. These updates provide the latest data about health workforce funding recipients working in and entering service in communities who need them. Updates also include alumni data, tracking clinicians who have completed their service contracts through HRSA workforce funding.
What’s New?
Updates Include:
- Applications and award recipients for health workforce loan repayment and scholarship programs:
- National Health Service Corps (NHSC)
- Nurse Corps
- Substance Use Disorder Treatment and Recovery (STAR)
- Pediatric Specialty
- NHSC, Nurse Corps, and Graduate Medical Education alumni data
- Downloadable data files on health workforce programs in the HRSA Data Warehouse
|
|
SFY 2026 Specialized Docket Subsidy Project Funds
The Ohio Department of Behavioral Health (DBH), Office of Criminal Justice and Recovery Services, Bureau of Criminal Justice, has announced that Specialized Docket Subsidy Project Funds will be available to operational specialized dockets that are currently certified (initial or final) by the Supreme Court of Ohio and are not currently receiving funding from the Specialized Dockets Subsidy Project. The funding will be available for the period of July 1, 2025, through June 30, 2026 (SFY 2026).
Funds supporting this project are granted based on an estimate of state and federal funds for mental health and addiction services in Ohio. Should funding be reduced below the estimated level, the amount of funds approved for this project may be reduced or terminated per written notice to the applicant by DBH. Please note: These funds can be retroactively applied for allowable expenses incurred on or after July 1, 2025.
Note: Courts that operate specialized dockets currently receiving funding through this initiative may apply for funding if said courts are applying for a different specialized docket project that is not receiving these funds.
Interested applicants should submit an expression of interest email to [email protected] by 3:00 p.m. on March 31.
View the full EOI here. |
|
OneOhio Regional Grant Cycle 2 Now Open
The OneOhio Recovery Foundation Regional Grant Cycle 2 is now open, with applications currently being accepted through their Grant Portal. Funding Inquiries are due in the portal by February 11, 2026. Applicants can access the web portal at the OneOhio Regional Grant Headquarters webpage, which includes additional information and resources.
Regional Grant Cycle #2 Schedule:
- Wednesday, December 10: Regional Grant Cycle 2 RFP posted on the Grant HQ
- Wednesday, January 14: Regional Grant Cycle 2 Funding Inquiry window opens
- Wednesday, February 11: Regional Grant Cycle 2 Funding Inquiry window closes
- March – May: Region Grant Reviewers review Funding Inquiries and prepare recommendations for the OneOhio Regional Boards
- Friday, May 29: Deadline for Regional Boards to approve funding recommendations and submit them to the Foundation
Grant Cycle 2 Webinars:
- RFP Webinar - Tuesday, December 16 & Wednesday, January 7 [View Recording]
- Funding Inquiry Webinar - Wednesday, January 21 [View Recording]
- Impact Academy - Evidence Guide for Applicants, Tuesday, January 27 [Register Here]
View the Request for Proposals (RFP) and Funding Priorities information here. |
|
Ohio General Assembly Update
There has not been any legislative activity since lawmakers adjourned in December. Ohio House Members are not scheduled to return to the statehouse until mid-February and Ohio Senate committees were cancelled due to weather conditions this week. When lawmakers do return for the 2026 legislative session, they are expected to focus on a Capital Budget and/or Medicaid funding shortfall, fraud waste and abuse oversight activities, additional property tax reforms, and possibly another corrections bill to adjust spending and minor policy issues. Because this year is an election year, lawmakers will be away from the statehouse for significant periods of time for both the primary and general election campaign periods. Of course, Ohio Council staff will continue to review and monitor legislative activity, engage lawmakers and key staff, and advocate with DeWine administration officials on policy issues that affect the community behavioral health system. Accordingly, below are legislative measures that we have identified for further review and monitoring.
|
Bill
|
Bill Sponsor and Description
|
Current Status
|
|
HB 28
|
ELIMINATE REPLACEMENT PROPERTY TAX LEVY AUTHORITY (MATHEWS A, HALL T) To eliminate the authority to levy replacement property tax levies.
- Concerned about impact on local levies
- Included in Budget Bill
- House and Senate voted to override Gov’s veto
|
4/8/25 – Passed House, Pending in Senate Committee
*Included in HB 96
10/2/25 veto overridden and now law.
|
|
HB 58
(Changed from opposition to IP)
|
RECOVERY HOUSING Reform (PIZZULLI J, JARRELLS D) To reform regulatory system of recovery housing residences.
- Sub Bill accepted with positive changes – removes the following measures: certificate of need; bed fees; and ADAMHS board investigations of recovery residences.
- We are continuing to work with ORH and OARP to improve the bill
|
11/18/25 – House Community Revitalization Committee (5th Hearing)
*Accepted Sub Bill
|
|
HB 96
|
Operating Budget for SFY 26-27 (Stewart) to make appropriations for the biennium, levy taxes, and provide authorization for state programs.
- Passed GA 6/25; Gov Signed 6/30 – appropriations effective immediately; other provisions 9/30.
- Awaiting guidance on federal Medicaid changes (work requirements and redetermination process; MHAS block grants.
- Items not included Peers to CDPB; QMH credential; Tax increase on Marijuana and Sports Gaming
|
6/25/25–Enacted by General Assembly; 6/30/25-- Signed by Governor with 67 vetoes. Eff 9/30/25
10/2/25—GA voted to override one veto item (repeal of replacement levy)
|
|
HB 160
Consolidated into SB 56 conference committee report
11/19/25
|
REVISE LIQUOR CONTROL, HEMP, MARIJUANA LAWS (STEWART B) To revise specified provisions of the liquor control, hemp, and adult-use marijuana laws and to levy taxes on marijuana.
- Combines regulations and oversight responsibilities of recreational and medical marijuana into the Division of Marijuana Control (DMC).
- Reduces THC levels; imposes marketing, advertising and informational safeguards; prohibits use in public.
- Modifies how revenue from the 10% tax on adult-use marijuana is credited by dedicating 20% of the revenue to make temporary payments to municipalities and townships and redirecting the rest to the GRF.
Lawmakers to address in fall legislative session
|
5/7/2025 - House Judiciary, (Third Hearing)
|
|
HB 162
|
Regarding Minors’ Medical Records (Click)Related to medical records of minors and parental consent.
- Requires a health care provider to ensure a minor’s parent or guardian has access to the minor’s EHR to the fullest extent permitted under HIPAA; and offer opportunities and reminders about consent.
|
10/15/2025 -PASSED HOUSE; 10/22/25 -referred to Senate Health committee
|
|
HB 172
(Oppose)
|
REQUIRE PARENTAL CONSENT-MINORS' MENTAL HEALTH SERVICE (NEWMAN J) To prohibit the provision of mental health services to minors without parental consent.
- Would repeal section 5122.04 (temporary emergency counseling authority)
- Teresa testified in opposition in committee along with a host of other advocates
|
11/19/2025 - House Health (Third hearing)
|
|
HB 184
|
Budget Corrections bill (NF reimbursement payment recalculation) (Stewart B) – originally a bill to address collegiate NIL contracts, the bill was used as the vehicle for a budget corrections bill.
See LSC summary
|
11/19/25 – Passed House and Senate. Sent to Governor for signature.
|
|
HB 189
|
REGARDING SCHOOL BEHAVIORAL THREAT MANAGEMENT (HALL T, GHANBARI H) Regarding a statewide behavioral threat management operational process for public and chartered nonpublic schools.
- Monitoring for significant changes and added requirements for providers working in schools
|
4/29/2025 - House Education (1st hearing)
|
|
HB 190
|
PUBLIC SCHOOLS-GENDER PRONOUN USE (NEWMAN J, WILLIAMS J) To enact the Given Name Act regarding the use of gender pronouns in public schools.
- Monitoring for new requirements and possible penalties for providers operating in schools and working with students.
|
4/29/2025 - House Education (1st hearing)
|
|
HB 219
|
ESTABLISH INSURER NETWORK ADEQUACY STANDARDS (DEETER K) To establish network adequacy standards for health insurers.
*LSC Analysis
|
10/7/2025 - House Insurance, (Second Hearing)
|
|
HB 220
|
REGARDING PRIOR AUTHORIZATION REQUIREMENTS (WORKMAN H) Regarding health insurance and Medicaid program prior authorization requirements.
*LSC Analysis
|
10/28/2025 - House Insurance, (Third Hearing)
|
|
HB 309
|
LAW CHANGES-COUNTY BUDGET COMMISSIONS (THOMAS D) To modify the law governing county budget commissions and property taxation.
|
11/19/2025 - Consideration of Senate Amendments; House Does Concur, Vote 64-25; Pending Gov’s signature.
|
|
HB 335
|
LIMIT INSIDE MILLAGE REVENUE INCREASES – (Thomas) To limit revenue increases from inside millage levies occurring due to a reappraisal or update, to allow a reduction of inside millage to accompany a school district income tax levy, to allow a reduction of inside millage to accompany a municipal income tax levy, and to require county budget commission approval of inside millage reductions to accompany a county sales tax levy.
*Monitoring for impact on local human services levies
*Governor has established Task Force to study property tax reform and submit report
*LSC Analysis and *Comp Doc analysis
|
11/19/2025 – House Concurs with Senate amendments, Pending Gov’s signature
|
|
HB 346
|
CHILD ABUSE MANDATORY REPORTING (KISHMAN M, WILLIAMS J) To require mandatory reporters of child abuse or neglect to report to both a peace officer and the public children services agency.
*Working with other stakeholders to express concerns about duplication and educating lawmakers on reporting process.
|
11/12/2025 - House Public Safety, (Second Hearing)
|
|
HB 393
|
COMMUNITY CORRECTIONS-OBTAINING ID CARDS (CLICK G, BREWER D) To require that community-based correctional facilities and programs assist inmates in obtaining state identification cards prior to release.
|
11/19/2025 – Passed by House (89-0)
|
|
HB 455
|
Elimination Obsolete Educational Provisions (Manning / Bird)
Regarding the operation of public schools and elimination of obsolete provisions of education law.
- Revises the procedures for public schools’ parental notification of several issues, including (2) services related to a student’s mental, emotional, or physical health or well-being
|
11/19/2025 – Passed by House (87-0)
|
|
HB 508
(Support)
|
LAW CHANGES-APRN PRACTICE (GROSS J, BAKER R) To modify the laws governing the practice of advanced practice registered nurses and to name this act the Better Access to Health Care Act.
- Grants an APRN the option to practice without a
- standard care arrangement and collaborating practitioner if the APRN has practiced in a clinical setting for 5,000 hours.
- Submitted proponent testimony
|
11/18/2025 - House Medicaid, (Third Hearing)
|
|
HB 515
|
ADAMH BOARD COMPOSITIONS, CONTRACTS (WILLIAMS J) Regarding the composition of boards of alcohol, drug addiction, and mental health services and regarding board contracts.
- Requires political affiliation to be considered for Board appointment;
- Includes new language regarding a Boards’ contracting authority: “No board shall deny a contract to or refuse to contract with a for-profit entity or nonprofit entity, including a faith-based entity, based solely on the entity's for-profit or nonprofit status.”
|
10/15/2025 – Referred Committee House Children and Human Services
|
|
SB 1
|
ADVANCE OHIO HIGHER EDUCATION ACT (CIRINO J) To enact the Advance Ohio Higher Education Act regarding the operation of state institutions of higher education
- Similar to SB 83 from last GA (Companion to HB 6)
Allows waiver for professional licensure requirements for social work; counseling; and other healthcare classes.
|
3/28/25 – Enacted.
Signed by Governor DeWine. Effective June 30, 2025
|
|
SB 7
(Support)
|
REGARDING INSTRUCTION-SUBSTANCE USE (JOHNSON T) Regarding instruction for public and chartered nonpublic school students in the harmful effects of substance use.
- Reaching out to sponsor to discuss prevention generally and express support; Senator Johnson is also sponsor of SB 105 (ADAMHS board bill) from last GA
|
4/30/2025 – Passed by the Senate; 9/30/25 – First Hearing in House Ed Committee
|
|
SB 56
*Vehicle used to consolidate marijuana rules along with Intoxicating Hemp regulations
|
LAW CHANGES-MARIJUANA, LIQUOR, HEMP – (Huffman) To revise specified provisions of the liquor control, hemp, and adult-use marijuana laws, to levy taxes on certain hemp products, and to make an appropriation.
*10% tax on marijuana sales; distributes revenue to (36%) to local governments and remaining (64%) to state GRF
*Modifies regulations of Intoxicating Hemp products, including THC beverages to be compliant with new federal rules.
*See LSC Summary of Conference Committee Report
|
House Accepts Conference Committee Report, (Vote 52-34); Pending Senate passes Conference Report 12/9/25. Sent to Governor for signature – effective in 90 days once signed.
|
|
SB 86
Consolidated into SB 56 conference report.
|
REGULATE HEMP, CANNABINOID PRODUCTS (HUFFMAN S, WILKIN S) To generally prohibit the sale of intoxicating hemp products, except for sales at licensed dispensaries; and to levy taxes
- Many provisions of this bill have been included in SB 56
|
5/7/25 – Passed Senate; Pending in House General Govt Committee (5th hearing)
|
|
SB 138
(Support)
|
MODIFY ADAMH SERVICES LAWS (JOHNSON T) To modify various laws regarding boards of alcohol, drug addiction, and mental health services and to impose penalties for not registering recovery housing residences.
- Compromise language approved by the OC Board
- OC, OACBHA and OARP support
- Added criminal penalties for recovery residence violations
|
7/1/25 – Signed by Governor; effective 9/30/25.
|
|
SB 160
|
REGARDING PRESCRIPTION DRUGS-MEDICATION SWITCHING (LISTON B, JOHNSON T) Regarding prescription drugs and medication switching.
- Prohibits insurers from making mid-year drug formulary changes that disrupt physician’s ability to exercise medical expertise to help their patients.
|
10/21/2025 -- Senate Financial Institutions and Insurance (third hearing.
|
|
SB 162
|
REGARDING HEALTH INSURANCE RECOUPMENT (BLESSING III L) Regarding the timeframe for health insurer recoupment from health care providers.
- Changes 24-month takeback timeframe, decreasing it to the same timeframe given to a provider to submit a claim, and also prohibit insurers from changing these timeframes during a contract period.
- Would prohibit insurers from charging a provider for appealing a determination of overpayment.
|
10/21/2025 - Senate Financial Institutions and Insurance (First Hearing)
|
|
SB 164
|
REGULATE ARTIFICIAL INTELLIGENCE-HEALTH INSURERS (CUTRONA A) Regulate the use of artificial intelligence by health insurers.
- Requires transparency by insurers on the use of AI tools in prior authorization determinations and ensures that determinations are made through review of individual merits of claims by licensed clinical professionals.
|
10/28/2025 – First hearing Senate Financial Institutions and Insurance
|
|
SB 165
|
PROHIBIT HEALTH INSURERS-CERTAIN CLAIM DENIALS (MANCHESTER S) To prohibit a health insuring corporation from reducing or denying a claim based on certain factors.
- Contains prohibitions on down-coding for all providers, including prohibitions on limitations on reimbursement for time spent with patients.
|
10/14/2025 - Senate Financial Institutions and Insurance (First hearing
|
|
SB 166
|
PROHIBIT FEES-HEALTH INSURER, MEDICAID ELECTRONIC CLAIMS (MANNING N) To prohibit fees for electronic claims submission by health insurer and the Medicaid program.
- Would prohibit insurers from imposing a charge or fee, (including through withholding from payment), on any provider for electronic fund transfers or remittance advice transactions.
|
4/2/2025 - Referred to Committee Senate Medicaid
|
|
SB 197
|
VARIOUS CHANGES-INTERNET GAMBLING (MANNING N) To legalize internet gambling and levy a tax on businesses that provide internet gambling, to permit internet lottery gaming and online wagering on horse racing.
- Authorizes three new types of online gambling: internet gambling, lottery gaming, and online horse racing.
- Consolidates the regulation of gambling in Ohio under the authority of the Ohio Casino Control
- These provisions were not included in the budget bill
|
5/28/2025 - Senate Select Committee on Gaming, (Third Hearing)
|
|
SB 258
(Support)
|
BETTER ACCESS TO HEALTH CARE ACT (LANG G, ROMANCHUK M) To modify the laws governing the practice of advanced practice registered nurses
*Companion bill to HB 508
*Requires 2000 hours of practice in a clinical setting to practice without a SCA (most likely gets amended to 5000 hours)
*Sen. Romanchuk stated that bill is pending action on HB 508.
|
10/1/2025 - Referred to Committee Senate Health
|
|
SB 274
(Oppose)
Had positive discussion with Sen. Brenner. Bill not on fast-track. IP meetings expected in new year.
|
PROHIBIT MENTAL HEALTH SERVICES WITHOUT PARENTAL CONSENT (CIRINO J, BRENNER A) To prohibit the provision of mental health services to minors without parental consent.
*Companion bill to HB 172
*Removes 5122.04
|
10/1/2025 - Referred to Committee Senate Health
|
|
SB 276
|
INTERSTATE COMPACT-SCHOOL PSYCHOLOGISTS (ROEGNER K) To ratify the Interstate Compact for School Psychologists.
|
11/12/2025 – Passed Senate; 11/19/21 – Referred to House Education
|
|
SB 295
|
RESTORATION OF COMPETENCY-CRIMINAL(MANNING N, PATTON T) Relative to the timeline for restoration of competency in criminal cases and to declare an emergency.
- Increases the time during which a criminal defendant may be held for purposes of restoring the defendant’s competency – up to 5 years in some instances;
- Tolls or restarts the time limit for restoration of competency under certain circumstances.
- Retroactive to any criminal defendant found incompetent to stand trial prior to the effective date of the bill and whose restoration to competency is ongoing or whose case remains pending.
|
11/12/25 – Passed Senate (31-0); 11/19/2025 - Referred to House Judiciary Committee
|
|
|
Ohio Adopts 5 New Property Tax Reforms
Governor Mike DeWine has signed into law a package of property tax reform legislative measures that will impact local governments and schools’ options to generate revenue for community programs. Those bills include:
- HB 124 – Property Tax - Thomas, D. Hall, T. - To modify the process for making property tax sales-assessment ratio studies. - Signed: December 19, 2025, Effective: 90 days
- HB 129 – School District Millage - Thomas, D. - To generally include fixed-sum levies in the calculation of a school district's millage floor and to authorize, with limitations, school district fixed-sum levies. - Signed: December 19, 2025, Effective: 90 days
- HB 186 – School District Revenue - Hoops, J. Thomas, D. - To authorize a reduction in school district property taxes affected by a millage floor that would limit increases in such taxes according to inflation, to modify property tax reductions for residential property, to modify the process for certifying property tax abstracts, and to make an appropriation. - Signed: December 19, 2025, Effective: 90 days
- HB 309 – County Budget Commissions and Property Tax - Thomas, D. - To modify the law governing county budget commissions and property taxation. - Signed: December 19, 2025, Effective: 90 days
- HB 335 – Property Tax Overhaul - Thomas, D. - To limit revenue increases from inside millage levies occurring due to a reappraisal or update. - Signed: December 19, 2025, Effective: 90 days
The Ohio Council will keep members informed of any presenting impacts of these changes, or future actions related to property tax reforms. |
|
WorkOhio Launched to Provide Personalized Support to Job Seekers
Lt. Governor Jim Tressel announced the launch of WorkOhio – a new initiative to connect Ohioans with in-demand jobs through personalized support from teams of regional job experts. The intention is to help Ohioans find great jobs, especially in high-demand fields.
WorkOhio serves as a “front door” to these resources, allowing Ohioans to navigate the job tools that fit them best, all in one convenient online location. At the center of WorkOhio is a new website – WorkOhio.gov – an easy-to-use starting point for anyone looking for new job opportunities, training programs, or other resources aligned with their background, experience, and goals. On the website, Ohioans can select the region where they live or want to work. From there, they can submit a short contact form requesting one-on-one support and a job expert who lives in their region will connect with them within two business days. WorkOhio is free and no login is required.
WorkOhio also supports users who prefer to explore on their own. The website offers resources and guidance tailored to different stages of life and career paths – helping job seekers of all backgrounds quickly find the job tools most relevant to them.
Read the full announcement here. |
|
CDCA-Pre & CDCA Requirement Changes Coming in 2026
To strengthen the foundation and ensure consistency of substance use disorder counseling education, changes will be made in 2026 to what will be accepted to apply for initial CDCA Preliminary and CDCA certifications.
Effective March 1, 2026 – the Ohio Chemical Dependency Professionals Board (CDP) Board will no longer be accepting single CEU’s or CEU packages for initial applications and will only be accepting college courses OR a CDP Board approved continuing education CDCA Bundle.
These changes will also improve efficiency of CDCA application reviews.
For further information, please click here CDCA Certification Changes
Any questions about these changes or Educational Providers interested in submitting a Bundle, please contact Esha Thakar @ [email protected]. |
|
Ohio Becomes 3rd State to Enter Counseling Compact
The American Counseling Association (ACA) has announced that Ohio is the latest state to begin granting privileges under the Counseling Compact, marking another significant milestone in expanding access to mental health care. This development means Licensed Professional Clinical Counselors in Ohio can now practice across state lines, helping to bridge gaps in care and bring vital services to communities in need.
Ohio is joining Arizona and Minnesota in the compact, with other states expected to continue adoption. To date, 38 states and the District of Columbia have ratified the interstate agreement. The ACA asserts that once fully ratified, the compact would give an estimated 122 million people in the U.S. who live within Mental Health Professional Shortage Areas easier access to mental health supports.
The compact is a legislative agreement among participating states that allows professional counselors to practice across state lines either in person or via telehealth. It is a mutual recognition model that functions much like a driver’s license — participating states agree to recognize the license of all eligible counselors from other compact states, allowing them a privilege to practice. Previously, counselors have had difficulty transferring their licenses from one state or jurisdiction to another because of the independent nature of jurisdictional licensing rules and regulations. There was little consistency regarding the requirements for licensure, and these varying requirements make it difficult to transfer one’s license.
States and jurisdictions that have passed Counseling Compact legislation include: Alabama, Arizona, Arkansas, Colorado, Connecticut, Delaware, Florida, Georgia, Indiana, Iowa, Kansas, Kentucky, Louisiana, Maine, Maryland, Minnesota, Mississippi, Missouri, Montana, Nebraska, Nevada, New Hampshire, New Jersey, North Carolina, North Dakota, Ohio, Oklahoma, Rhode Island, South Carolina, South Dakota, Tennessee, Utah, Vermont, Virginia, Washington, West Virginia, Wisconsin, Wyoming, and Washington, D.C.
To learn more, visit the ACA website and watch this video interview with ACA's Lynn Linde on what counselors can expect going forward. |
|
BOP Moving to Adopt Permanent Rules Banning Kratom
On December 12, 2025, Governor Mike DeWine signed Executive Order 2025-08D (EO), authorizing the Ohio Board of Pharmacy (BOP) to adopt emergency proposed changes to Ohio Administrative Code (OAC) 4729:9-1-01.1 Mitragynine-related compounds, designating all synthetic kratom compounds and other compounds derived from kratom as illegal, Schedule 1 drugs.
While the executive order allowed the emergency rules to go into effect immediately, those temporary rules authorized in the EO will expire on June 10th, 2026. As such, the Ohio Board of Pharmacy is moving forward through the JCARR process to make permanent this rule and proposed making the primary compound in kratom as a Schedule I controlled substance in OAC 4729:9-1-01.1 and OAC 4729:9-1-01.2.
The Ohio Council submitted comments in support of the rescheduling of Kratom and Mitragynine-related compounds as a Schedule I drug. The proposed rules are consistent with well-established principles used to evaluate controlled substances, including high potential for misuse, the risk of dependence, and the absence of accepted medical use under regulated conditions. These factors, combined with risks to young people through early exposure, alignment with regulatory policies of similar substances, and clinical evidence shared by Ohio Council members of increased presentation of clients seeking detox and treatment for Kratom dependence, strongly supports reclassification.
Kratom is a plant found in southeast Asia, which has been marketed in Ohio and across the United States as an opioid alternative. Due to its unregulated nature, the effects of kratom vary depending on the dosage and manufacturer, and has been tested to reach intoxicating levels higher than morphine, raising numerous public health and safety risks. Kratom has recently been sold at convenience stores, gas stations, and other commercial locations with no age requirements or restrictions, making the substance easily accessible not only to adults but to young people as well.
While the emergency designation within the EO allowed immediate adoption of the BOP rules designating synthetic Kratom and Mitragynine-related compounds as a Schedule I drug, the permanent rules will continue to travel through the normal JCARR process.
The Ohio Council will continue to monitor any changes to these rules as the process continues to unfold and will keep Ohio Council members informed of any changes. |
|
Ohio SB 56 – Recreational Marijuana Signed into Law
Governor Mike DeWine has signed Ohio Senate Bill 56 (SB 56), while vetoing a provision of the bill that would allow the retail of THC beverages. SB 56 reforms some of the adult-use recreational marijuana programs and regulates other intoxicating hemp products.
The veto comes in response to Congressionally enacted requirements in H.R. 5371, which enacted a federal ban on intoxicating hemp beginning November 2026. This ban includes a ban on THC beverages containing intoxicating hemp. Governor DeWine asserted that continuing sales of intoxicating hemp beverages for the remainder of the year will create confusion for consumers and a lack of conformity with federal law.
Marijuana Tax Structure: The final bill maintains the current 10% adult-use marijuana tax rate, eliminates the voter-approved Cannabis Social Equity and Jobs Fund, allocates 36% of revenue from excise tax to the Host Community Cannabis Fund for local communities, and uses tax revenue to creates an expungement system for Ohioans who were convicted of low-level marijuana possession charges before Ohio passed legal possession. All remaining tax revenue will go to the general revenue fund.
Marijuana Provisions: The final bill criminalizes the possession of recreational marijuana bought outside of Ohio, and bars packaging targeted at children. Maximum THC levels in adult-use marijuana extracts are reduced from a maximum of 90% down to a maximum of 70%; and caps THC levels in adult-use flower to 35%. It also limits the number of active marijuana dispensaries and prohibits smoking in most public places. Left unchanged, however, are the number of home-grown plants that a person can possess, remaining at the original 6-plant limit per person, or 12 plants per residence.
Additional information including the line-item veto boxed text is below:
|
|
ODM Proposed Changes to Incident Management Rules
The Ohio Council recently submitted comments to the Ohio Department of Medicaid on a package of proposed updates to incident management rules including OAC 5160-44-05, 5160-26-14, and 5160-59-09. Together, these rules govern incident reporting, investigation, and follow-up responsibilities for Medicaid providers, managed care organizations, and OhioRISE care management entities. The proposed changes make needed clarifications across various Medicaid programs and create more consistency while meeting discrete federal requirements embedded in specific waivers or programs.
In our comments, we focused on implementation considerations, including clarity around incident notification requirements, appropriate involvement of providers following incident investigations, and the administrative burden created by overlapping reporting and oversight processes. We encouraged ODM to consider opportunities to align requirements across systems and reduce unnecessary duplication while maintaining appropriate safeguards for individuals served.
The Ohio Council will continue to monitor developments on this rule package and share updates with members. |
|
ODM Launches Medicaid Work Requirement Resource Page
The Ohio Department of Medicaid has launched a new webpage for professionals to find additional information on the Work and Community Engagement Requirements for Group VIII Medicaid Enrollees. Per HR 1, Federal Work and Community Engagement Requirements are slated to go into effect on January 1, 2027 – however there may still be some states may opting to adopt these requirements earlier.
Due to new federal laws, Medicaid eligibility requirements will be changing for individuals eligible for and enrolled in Group VIII coverage. The new rules will introduce a Work and Community Engagement Requirement for certain non-exempt individuals, ages 19 - 64, to demonstrate ongoing participation in work or community activities for a minimum of 80 hours per month as a condition of coverage.
The webpage includes:
- Group VIII Overview Information
- List of Qualifying Exemptions (including those with MH conditions or engaged in SUD Treatment)
- List of Qualifying Activities to Meet Work & Community Engagement Requirements
- Compliance Reporting Information
Clients can determine if they are part of Group VIII by logging in to their Self-Service Portal (SSP) account and looking on the “View My Benefits” page. They can also look at a recent notice from ODM if they do not use the Self-Service Portal.
ODM has stated that the webpage will continue to be updated as additional CMS guidance becomes available and advises that providers continue to check this page as we move toward implementation. ODM asks stakeholders to note that information published on this webpage is subject to change prior to implementation, based on CMS guidance.
Those who have questions or feedback can email [email protected]. |
|
Next Generation MyCare Ohio
The Ohio Department of Medicaid (ODM) launched the Next Generation MyCare program effective January 1, 2026, to better serve Ohioans who are dually eligible for Medicaid and Medicare. The program and all four Next Generation MyCare plans are now live in the existing 29 MyCare counties, with statewide expansion planned later this year.
Claims Submission Overview
As a reminder, all Next Generation MyCare claims must now be submitted via EDI through the Ohio Medicaid Enterprise System (OMES), also referred to as the “one front door” (OFD).
Effective 1/1/26, all MyCare claims must be submitted through the OFD, regardless of date of service. Claims will be routed to the appropriate plan based on the Receiver ID in the header of the EDI transaction, and the Payer ID in the 2010BB loop NM109. New Receiver and Payer IDs are published in the 837P companion guide. ODM sent trading partners an email with billing reminders on 1/7/26 outlining some common issues.
For Anthem, Buckeye, CareSource, and Molina, claims must be billed through the OFD effective 1/1/26 regardless of date of service. For claims submitted on or after 1/1/26, including claims with dates of service prior to 1/1/26, providers should submit claims through the OFD using the Next Generation MyCare Plan Payer IDs from the current companion guide, and the member’s MMIS (Medicaid ID) number. This applies even though the companion guide indicates the new payer IDs are for dates of service beginning 1/1/26.
Primary Payer Scenarios
The ODM MyCare FAQ (linked below) outlines claims submission requirements for various primary payer configurations.
Dual Benefit Members or Medicaid-Only Members (Medicaid is Primary):
- Submit EDI claims through the OFD to OMES.
- Use the member’s Medicaid ID (MMIS), even if other member IDs exist.
- Use the Next Generation MyCare Plan Receiver ID and the appropriate Payer ID in the 2010BB loop to ensure correct routing.
Medicare-Covered Services for Medicaid-Only Members (Crossover Claims):
- If Medicare is the primary payer, submit the claim to Medicare using your standard process. Claims for MyCare members will automatically cross over to the Next Generation MyCare plan.
- If a Medicare Advantage (Part C) plan is the primary payer, submit the claim to that payer first. After adjudication, submit the claim through the OFD using the appropriate Receiver ID and Payer ID for the Next Generation MyCare plan.
Please refer to the companion guides and FAQ for additional details.
Aetna and United Claims Runout
Aetna Better Health of Ohio and UnitedHealthcare are no longer MyCare Ohio plans as of December 31, 2025. However, both plans will continue to process and pay claims for up to 365 days following the end of the year and remain responsible for claims with dates of service through December 31, 2025. These claims should continue to be submitted directly to Aetna or United using existing processes. As a reminder, the MyCare Ohio contract is separate from the Ohio Medicaid Managed Care contract and United remains a Medicaid managed care plan through the UHC community plan, while Aetna retains the OhioRISE contract.
Outbound Transactions and Eligibility Lookups
ODM has also shared that the Next Generation MyCare plans are currently experiencing issues with outbound transactions, including the delivery of 277 Claims Acknowledgements (277CA) and 835 Electronic Remittance Advice (ERA) files, as well as with member eligibility processing through the Next Generation MyCare managed care 270/271 process. In addition, CareSource is experiencing issues impacting its ability to deliver outbound managed care 835 ERA files. The plans are actively working to resolve these issues. Once resolved, providers should begin receiving 277CAs and 835 ERAs through normal processes, and member eligibility lookups may resume through the standard Next Generation MyCare MCO 270/271 process. In the interim, providers may contact the plans directly to obtain claim adjudication status and 835 ERA information. Member eligibility can also be verified through Provider Network Management (PNM) or by using the fee-for-service 270/271 eligibility process.
The below resources are also helpful for providers.
|
|
Trump Issues EO Creating the Great American Recovery Initiative
On January 29th, the Trump Administration released an executive order, Addressing Addiction through the Great American Recovery Initiative, that is designed to coordinate the federal government response to the substance use and addiction crisis. While few details are available, this White House fact sheet, describes how this Initiative will advise federal agencies on how to integrate programs on drug prevention, early intervention, treatment, recovery support and reentry. It is also intended to increase awareness of the disease of addiction, help individuals access treatment, and foster a culture that celebrates recovery. The Initiative is also tasked with consulting states, Tribal nations, local governments, community and faith-based organizations, the private sector and philanthropic partners to identify effective recovery strategies to ensure more Americans receive life-saving care and support.
The Great American Recovery Initiative will be chaired by Department of Health and Human Services Secretary Robert F. Kennedy Jr., and Senior Advisor for Addiction and Recovery Kathryn Burgum, a substance use and recovery advocate and former first lady of North Dakota. More information is expected to be released in the next few weeks. |
|
Trump Issues EO Designating Fentanyl as a Weapon of Mass Destruction
The White House has issued an executive order (E.O.) formally classifying illicit fentanyl and its core precursor chemicals as “weapons of mass destruction” (WMD), asserting that the synthetic opioid’s lethality, the role of organized criminal networks in its distribution, and its threat to U.S. national security justify the designation.
The order directs federal agencies, including the departments of Justice, State, Treasury, Homeland Security and Defense, to coordinate enhanced investigations, prosecutions, asset actions, and threat-response efforts to counter the fentanyl threat. It characterizes fentanyl distribution by cartels and foreign groups as fueling violence and undermining domestic security and seeks to mobilize the full range of government tools against fentanyl manufacture and trafficking.
It is unclear how this E.O. might affect local/state law enforcement activities, or penalties for lower-level drug offenses. The Ohio Council will keep members informed of developments in this space. |
|
Trump Issues EO Rescheduling Marijuana to Schedule III Drug
President Trump signed an executive order directing the Attorney General to “take all necessary steps to complete the rulemaking process related to rescheduling marijuana to Schedule III of the CSA in the most expeditious manner in accordance with Federal law.” If fully adopted, marijuana would be scheduled on par with steroids and codeine medications mixed with Tylenol.
The move seeks to reclassify cannabis out of Schedule I, loosening limits on research and other regulations while stopping short of full legalization. Rescheduling will not happen automatically because of the order, as it will still need to be done through the federal rulemaking process.
The order will also make cannabis easier for Medicare and Medicaid recipients to get by introducing a model that would cover medically recommended products with CBD, a non-intoxicating compound that comes from hemp, a close relative of marijuana, at no cost for seniors. Medicare Advantage beneficiaries will be able to purchase regulated hemp-derived products. These benefits would start next year.
In the interim, CMS will begin collecting data on patients using cannabis products. Similarly, HHS will conduct research to improve access to products made with CBD, and White House Deputy Chief of Staff James Blair has been charged with working with Congress on improving access to CBD products. |
|
CMS Awards Rural Health Transformation Funding & ODH Releases RFPs to Begin Implementation
The Centers for Medicare and Medicaid Services (CMS) announced the Rural Health Transformation (RHT) Program funding awards to all 50 states. Ohio will receive a total of $202,030,262, the 25th highest total amount. However, according to an analysis by the Health Policy Institute of Ohio (HPIO), Ohio was awarded one of the lower amounts, coming in as the 46th-most funding per rural resident.
As a reminder, the RHT program was created as part of the HR 1, also known as the One Big Beautiful Bill Act, that was signed into law on July 4, 2025. The RHT will allocate $50 billion to states over five years, with half the award evenly distributed across all 50 states and half of the award based on state-submitted applications. States will need to demonstrate efforts to achieve the RHT application deliverables in coming years to continue to receive fundings as outlined in the legislation. CMS also announced the creation of a federal Office of Rural Health Transformation that will be led by Alina Czekai.
Governor DeWine has designated the Ohio Department of Health as the lead agency for the RHT program. You can find Ohio’s RHT application and resources here and you can sign up to receive notifications about RHT program activities. ODH has released two RFPs through OhioBuys to begin implementation of Ohio’s RHT program. Information on those RFPs are here: Rural Health Workforce Pipeline; Pathways Upskilling and Retention RFP
|
|
CMS Increases 2026 Federal Poverty Level Standards
The Centers for Medicare and Medicaid Services (CMS) has released their 2026 Federal Poverty Level (FPL) Standards Memo. These standards are applied to eligibility criteria for programs such as Medicaid and the Children’s Health Insurance Program (CHIP), and account for the increase in the Census Bureau’s current official poverty thresholds by the relevant percentage change in the Consumer Price Index.
In 2026, the CPI saw a 2.6% increase, which, after adjusting for inflation led to a slight increase in FPL standards. In 2025 the poverty guideline for a family of 4 in Ohio would have been $32,900, and in 2026 that number has increased to $33,000. Read the 2026 CMS FPL Standards memo here, or view the full guidelines in 42 U.S.C. 9902(2) here. |
|
|
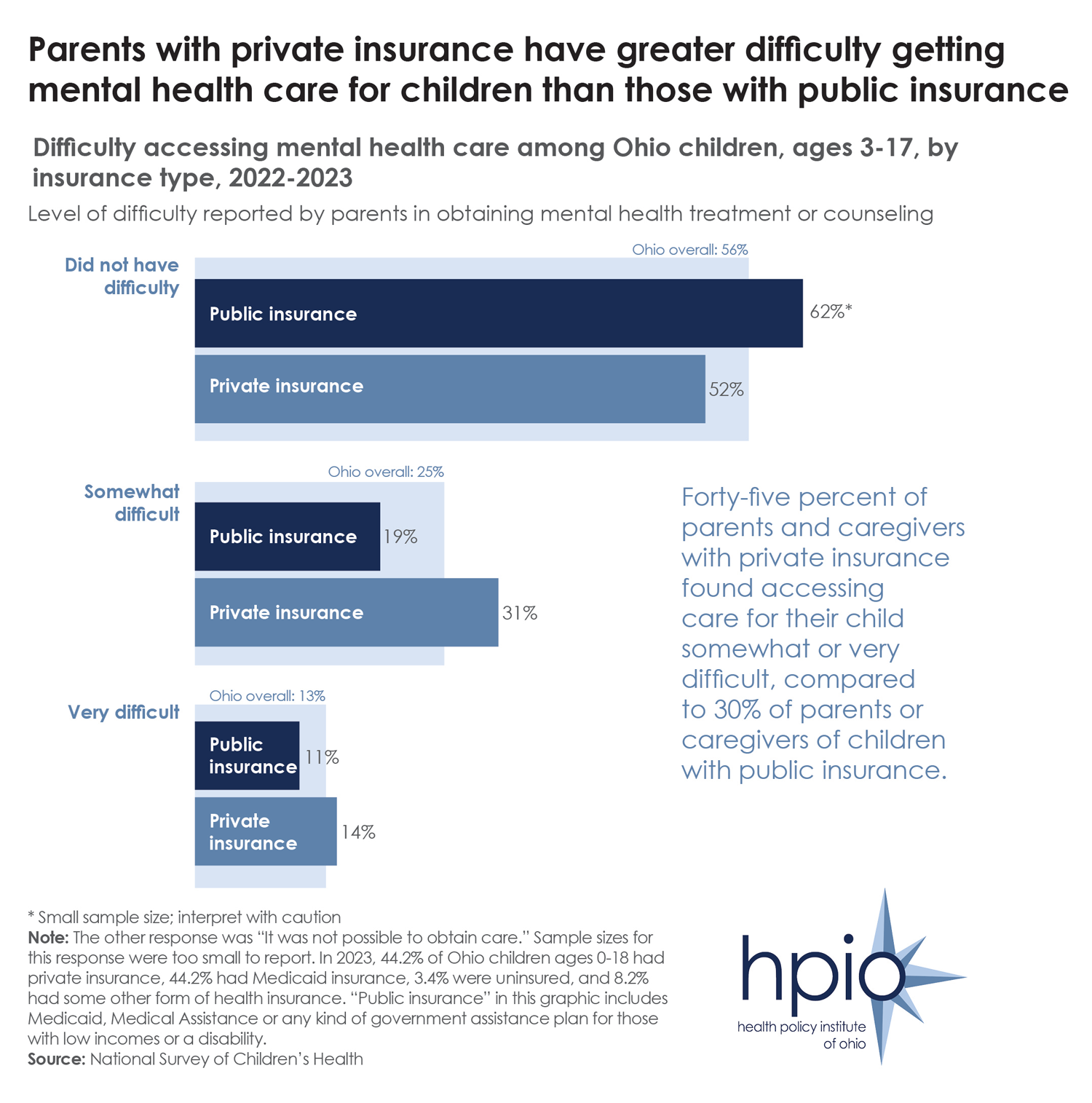{kind=link}
